
Secondary Hip Fractures among Aging Adults with a Previous Hip Fracture History: Cumulative 50 Year Overview, Analysis, and Possible Antidote as Observed from 1974-2026 Data Sources
Abstract
Hip fractures, which remain an immense public health concern, have been subject to study and prevention efforts for many decades, but with limited success in averting either incident, second or subsequent hip fractures, commonly attributed to a combination of age related proclivity to fall, low bone and muscle mass. This review examines second hip fracture incidence rates and determinants of this serious functionally debilitating injury as observed over time remains a current 2026 public health concern. It specifically explores if more preventive efforts are currently warranted in this regard, and in what respect, if indeed, more frail older adults are living longer, but may be in excessively poor health, fearful of moving or falling, malnourished, weak with poor balance, or depressed. Based on what is published, it is concluded 1) second hip fracture incidence rates remain considerable, especially among those who are frail with osteoporotic bone disease, poor vision, heart/or cognitive conditions, plus those with muscle deficits of the lower limb, live alone and have a falls history; 2) studies to identify possible mitigation approaches appear promising in this regard, along with more routine efforts to minimize falls risk and bone attrition.
Article Information
- Received
- Accepted
- Published
Copyright © 2026 Ray Marks
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Ray Marks, OARC Clinical Research and Education Director, Ontario L3T 5H3, Canada —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
In recent years, and despite some evidence of declining hip fracture rates in some spheres, it appears hip fractures continue to pose one of the most serious health care challenges facing policy makers, health care organizations, and older adults desiring to live independently in the community, rather than in the nursing home. Indeed, although some evidence of a decline in hip fracture prevalence has recently been reported e.g., 1, 2, 3, 4, the injury remains an ever present and potentially unwarranted cause of severe disability, excess morbidity, reduced life quality, post surgical hospital complications, and premature mortality among many older adults 4, 5, 6, 7, 8, especially men 3, and those of higher ages 9. Moreover, according to some, it is just as likely that the annual incidence of hip fractures could increase, rather than decrease over the next several decades 10, even though certain pharmacologic drugs may limit hip fracture risk. Due to an increase in the numbers of adults living to higher ages 9, a group not well studied, but where frailty and bone fragility prevalence rates continue to rise 11, 12, data projections may be underestimates if they do not commonly account for the fact that a ‘first’ hip fracture incident may be overlooked if the older adult does not have access to a hospital environment where data are collected and housed, or where only surgical cases are reported, rather than non surgically treated cases. In addition, falls, the second leading cause of an unintentional injury in adults 65 years or older, and that can lead to death as a result of a hip fracture may be overlooked as a factor of cost concern, and since, December 2019, possible COVID-19 acute and long term unresolved infections and related restricted access to health services or long waits for consultations. Costs may also be underestimated if they do not include actual hip fracture incidents occurring in isolated communities, where some adults may well have fallen and been unable to access help, or too fearful or ill to be admitted to a hospital. As well, even in areas where hip fracture rates have reportedly remained stable over 10 years, prior to COVID-19, rates of hip fracture did not appear to be falling in all locations 13, and recently appeared to be increasing among older women in Asia 5, China 10, Taiwan 14, Saudi Arabia 15, United States 16, and Costa Rica 17 and where the related loss of independence, mortality, and morbidity appears substantively and greater for women than for men 3, 18. Rates may also depend on multiple intrinsic as well as extrinsic factors including the location or region studied, the assessment tool and cut-off risk indicator levels, the availability of services, and whether data are systematically collected, accurate and up to date 19, 20.
At the same time, clearly stressing the need to continue to examine hip fracture trends, are increasing numbers of older adults at risk for falling, and sustaining an acute hip fracture, or a new fracture thereafter, which may be in the same location with a tendency to greater displacement or instability 21. Further, while Dolk in 1989 22 predicted the frequency of sustaining two hip fractures over the course of an individual's lifetime could reach 20 percent-this may have been an underestimate because the life span at that time was considerably lower than it is in 2026 and older adults such as those older than 80 years of age may not have been studied systematically. In addition, it is possible poor rehabilitation or oversight on remediating the causes of the initial fall or repeated falls may predispose the high age adult to a second hip fracture on the same or opposite side of the initial fracture, for example persistent bone fragility or undetected muscle imbalances or both. According to Shroder et al. 23 the risk of incurring a third hip fracture is not one that can be overlooked and in 1000 men appeared as high as 8.6 and at rates of 9.8 per 1000 for women, per year, or even higher 24.
Additional research reveals ipsilateral second hip fractures may include those that involve the trochanteric region that may not have been operated on, or in the case of internally fixated hips, may be attributable to the suboptimal placing of the surgical screw(s). Rarely, they may also occur after removal of internal fixation. However, in the study conducted by Shroder et al. 23 only 8 percent of second hip fractures occurred on the same side as the original fracture, while 92 percent occurred on the opposite side. Other data showed that 62 percent of those cases presenting with a femoral neck fracture and 72 percent of those with a trochanteric fracture, the two predominant hip fracture sites, were observed to have a preceding contralateral fracture of the same type. The mean time interval between the two fractures at the time of study was 3.3 years (range 5 days-14 years); although 20 percent incurred a second fracture within one year following the initial fracture, regardless of gender or fracture type, implying there is a very narrow window of opportunity to avert this event of an increased risk of a second hip fracture, which was shown statistically to be highly significant for both genders, but more marked for men.
Yamanashi et al. 25 who followed 714 hip fracture cases prospectively showed a second fracture, if it occurred, took place in general within eight months of the initial fracture, and was generally of the same type and strongly associated with the presence of senile dementia and/or a Parkinson’s disease diagnosis. It was not clear if these conditions had been treated with bone damaging drugs or others that may impede cognitions and motor control excessively along with the ability to avert a fall.
Nymark et al. 26 who assessed the average time period that commonly evolved from a first to a second hip fracture, if it occurred, was highest within the first 12 months following a first hip fracture. It was suggested preventive strategies at the time of a first fracture were strongly indicated as did Lönnroos et al. 27 who found the incidence rate for these second fractures were indeed quite high at one year post hip fracture surgery and even higher in the second year thereafter. Long term vigilance remains crucial however, as there may yet be a substantial risk of a second hip fracture among older adults within five years of the initial injury due to the persistence of a state of poor functional status 28, and that occurs more readily than not among those who survive unless concerted efforts are made to mitigate this risk 29.
However to date, despite the implementation of many community wide falls risk intervention programs in recent years, as well as the administration of bone mass building anti-osteoporisis medications, no strategy to date has proved widely successful in any sphere. Because the data span many decades and we may have overlooked some aspect of promise in this regard, we specifically sought to ascertain if indeed this is an area of current as well as future concern, and if so, what can be done in the present as well as future to avert an incident hip fracture epidemic as well as to foster or restore functional recovery post-hip fracture surgery in the case where a frail hip fracture patient has to undergo surgery.
The topic of second hip fractures and their known determinants was specifically highlighted and past as well as novel trends or potential intervention and prevention insights were specifically sought.
Although not as prevalent as primary hip fractures, second hip fractures may account for up to 15% of all hip fractures and immense suffering for many. Consequently, Guy et al. 30 proposed that concerted efforts be made to offset these events via early and consistent mitigation efforts, to avert related health costs, which may be greater than a single fracture event 31. In addition, poorly or sub-optimally treated hip fractures that result in fractures other than that at the hip will likely add to the ensuing level of functional disability that arises post hip fracture, and may foster an even more debilitating state unless addressed in a timely way. Hospitalizations also expose elderly patients to infectious agents even if timely surgery and rehabilitation strategies for restoring functional recovery post-hip fracture surgery are available, thus more preventive efforts to secure the health and safety of the older community dwelling adult in and out of the hospital remains strongly indicated.
Method and Procedures
To fulfil the aims of this report, all pertinent full length published studies in the English language detailing second and incident hip fractures as housed in the PUBMED,GOOGLE SCHOLAR, plus PubMed Central data bases over the time periods January 1 1970-May 31 2026, employing the key words: ‘Hip fracture’, ‘Older adults’, ‘Second hip fracture’. Summarized are pre and post pandemic findings pertaining to second hip fractures as published in peer reviewed research journals over this lengthy period during which researchers have shown considerable well founded concerns related to this topic area so as to discern trends and imperatives in this regard. Mitigation offered in the context of the preventive directives against second hip fractures were also sought in the desire to conceptualize how or reduce the immense hip fracture burden and its projected increase in incidence and prevalence in the near future. Those articles listed but failing to discuss first or second hip fractures or second hip fractures in the elderly, as well as those discussing fractures in the context of specific diseases or peri-prosthetic fractures, were excluded.
Results
Among the relevant studies published to date, while not all countries have reported on this topic, those that have including China, Costa Rica, Denmark, Finland, Ireland, Japan, the Netherlands, Norway, Spain, Turkey, the United States, the United Kingdom, and Taiwan appear to present findings that are quite comparable as a whole as regards incidence rates and possible risk factors for first and second hip fractures, regardless of their non-uniform analytic approaches, study periods, and follow-up durations 32.
Most detailed articles however, stem from research reports that date back to the 1970s up until 2020, but show much less visibility to date in 2026. In this regard, many current hip fracture reports focus on surgery repair as the treatment strategy of preference and advocate possible best practices for doing this, but very few refer to secondary fractures of the hip joint, and even in the case of primary fractures very little focus on their prevention in any regard. However, for more than 60 years, as discussed per Atik et al. 32, this current topic of interest that has prevailed since at least 1974, still remains problematic in 2026 and does not appear to have improved in any way or to any meaningful degree. This is possibly attributed to the presence of a persistent senile osteoporotic state, and related ongoing systemic weakening of the skeletal system among some older adult and not others 33, 34 that may result in a cumulative incidence rate of second hip fractures of 5.08% at one year, and 8.11% at two years after the first fracture and especially among those using psychotropic drugs. It has been further concluded however, that this situation will not improve without efforts to assure adequate and timely treatments to minimize osteoporosis, as well as more attention toward reducing inappropriate drug usage in the vulnerable older adult 27, as well as possibly targeting those exhibiting senile dementia and Parkinson's disease preferentially 25.
As affirmed by Chen et al. 28 who found almost 10 percent of hip fracture cases may develop subsequent hip fractures, as well as related increases in age specific mortality rates, those at most risk appeared to be women, and those who were obese, or had a cardiovascular condition. In addition, prolonged psychotropic medication usage, and poor vision were common risk determinants. In a systematic review of 13 case control studies conducted by Liu et al. 35 concerning risk factors for a second contra-lateral hip fracture this group indicated that among the risk factors in this respect were age, being female, having poor vision, a cardiac disease history, dizziness, and respiratory problems. Additional work by Egan 36 and Matani et al. 37 similarly identified older age, cognitive impairment, low bone mass, impaired mobility, plus vision, having a falls history and poor self-perceived health, dementia, and respiratory disease tended to heighten the risk for a second hip fracture.
As a result of these findings, and those of Lee et al. 38, early community based falls and fracture prevention program efforts plus ongoing support for extended time periods of post hip fracture rehabilitation are indicated to offset a probable 2-7 fold risk of a second hip fracture within 6 years, plus a higher mortality rate at one year compared to those with single hip fractures. This outcome prevails in particular if the primary fracture patient is a 55- 64 year old woman 39, 40 who has not received pharmaceutical treatments to counter osteoporosis, an intervention recommended by Kok et al. 41 to help reduce the incidence of primary as well as second hip fractures 42 such as vitamin D and calcium supplements.
In sedentary aging societies in particular, therefore, we would argue, practitioners and agencies must remain vigilant in this respect, because as indicated by Olmsland et al. 43 who found total hip fracture rates declined in both genders between 1999-2008, the rates of second hip fractures did not change. Bynum et al. 44 concluded secondary fracture prevention strategies that take a population perspective are indeed strongly indicated, to avert the possible impact of a second hip fracture that accounts for an increasing proportion of hip fracture surgeries, more demand on shrinking health care resources, poor outcomes and excess mortality rates 30, 38.
As per Sheik et al.45 efforts to improve screening for hip fracture patients at risk for subsequent fractures may be helpful, as may attention to older adults with signs of dementia, chest or urine infections and the presence of multiple chronic illnesses.
The disabling nature of the second hip fracture in all venues studied may however be difficult to avert in the event bone protection medication regimens have not been implemented in the past or peri operatively to any degree 46, 47. Indeed, cases deemed to have sustained a fragility fracture showed of those who survived surgery, 12.4% sustained a second hip fracture 48. The predisposing factors in this regard were identified as: being female, having a high bone fragility score, and a low physical capacity level. Vitamin D recommended for treating osteoporosis at safe levels was observed as having been implemented in only 24% of cases and 42% had ionized calcium levels below the reference range. The risk of death is higher after the second hip fracture, regardless of age and may be due in part to the lack of adequate post-surgical anti-osteoporosis medication recommendations or similar approaches at any time prior to the index hip fracture incident.
Zidrou et al. 49 who confirmed a second hip fracture can indeed occur quite commonly among older adults who have already suffered an initial hip fracture, indicated the key determinants in this regard were advanced age, being female, living alone, being demented, having a chest and/or urinary tract infection, chronic heart failure, and peripheral vascular disease. Other determinants of debilitating second hip fractures are cardiovascular conditions and signs of dementia 50, 51.
Unsurprisingly, older adults who incur a second hip fracture are found to have an increased mortality rate when compared to those with a single fracture 34, 52. As well, they are more than likely to have exhibited a history of fragility fractures, the need for assistance when walking outdoors and a history of falls, implying some, if not all secondary hip fractures may have been prevented by intervening accordingly. However, while high age adults who sustain a first hip fracture are at high risk of fracturing their other hip, preventive therapy is often not forthcoming 53. Yet even though many risk factors for a second as well as primary hip fracture are well documented, they do not appear to be clearly understood or integrated into efforts to mitigate against the risk of sustaining one or more hip fractures. These include the role of declines in bone mineral density, muscle size and density, and a possible lack of strategies other than anti osteoporosis interventions to meet these health challenges 54.
Ren et al. 61 who conducted a systematic search of hip fracture determinants showed significant risk factors for this included having a reduced hip muscle density, a reduced bone mineral density at hip femoral neck, and intertrochanteric regions, osteoporosis, signs of muscle degeneration and cognitive impairments, and calcium/vitamin D deficiencies. Among these, muscle morphology impairments, and calcium/vitamin D deficiency were deemed key deterministic factors.
Blattner et al. 63 who investigated the incidence rate, timing, survival time, mobility, and daily activity outcomes of second contralateral hip fractures using a matched pair analysis, found that of 1,933 patients, 148 (7.6%) sustained a second contralateral hip fracture on average within 2.2 years, with 40% occurring within the first postoperative year. Time to death after the second fracture was significantly lower for the cohort of patients with a single hip fracture (18% vs. 33%, p < 0.03) and within two years: 37.9% vs. 48%. Patients with second hip fractures demonstrated a significantly lower Barthel Index (66.7 vs. 77) and Parker Mobility Score (5.39 vs. 6.84) at follow-up, indicating reduced independence and mobility. Discharge to rehabilitation (possibly indicating slow recovery) after the first fracture was associated with a higher risk of subsequent fracture (58.1% vs. 49.3%). The authors concluded second contralateral hip fractures are under- recognized events that significantly reduce long-term mobility, independence, and survival time post-fracture within two years after the initial fracture, thus highlighting a critical window for targeted monitoring, falls prevention, and optimized osteoporosis management. They further concluded early identification of high-risk patients, especially those discharged to rehabilitation, was likely to be essential in efforts to mitigate any projected excess functional decline and premature mortality risk.
Tao et al. 77 propose since the level of fall risk perception among elderly hip fracture patients may only be moderate, clinical nursing staff may need to tailor interventions based on the patient’s intrinsic perceptions, as well as their heterogeneous profile, in order to provide precise targeted treatment strategies to reduce their’ falls risk and ultimately the actual risk of recurrent injurious falls.
In sum, despite almost 6 decades of research, including multiple efforts to identify upstream risk factors for incident as well as second hip fracture injuries, these remain sufficiently common and continue to cause sizeable percentages of older ambulatory adults, excess disability if they survive surgery 6, 55. This finding is not spurious, but remarkably consistent across multiple venues housing the most advanced orthopedic facilities in multiple regions of the globe renowned for their advanced health care and surgical practices. What is apparent is that among the reasons examined to explain this possible incident as well as second hip fracture risk, is not the surgical processes per se, but the possible failure to provide comprehensive multi dimensional preventive care approaches pre as well as post-hip fracture surgery, along with the patients’ functional and nutrition status, and ability to understand their important role in the recovery process 6, 55, 56, 58, 77, 78.
As such, and among possible solutions, preventive strategies at the time of the first hip fracture that aim at both averting any untoward immediate effects, as well as fostering those with disabling impacts may be desirable 26 and appear warranted for periods of up to 12 months in the case of men and 19 months in the case of women. Post operative rehabilitation and efforts to heighten activities of daily living and nutrition and gait 78 are especially indicated among, other approaches as outlined in Table 1.
Table 1. Possible approaches that might be harnessed to foster the prevention of incident as well as subsequent hip fractures among older adults living in the context of a community setting.| Possible Hip Fracture Mediators | Preventive Recommendations |
| Balance capacity | Foster balance/ambulation training |
| Bone mineral density attrition/fragility | Optimize bone health, prevent trauma |
| Cardiovascular disease history | Monitor cardiac status periodically |
| Cognitive status | Foster self- and coping efficacy, personal agency |
| Falls history/risk profile | Vigilance, education, control comorbid illnesses |
| Fear, depression | Counseling |
| Health status | Foster stress control, mobilize social support |
| Medication usage/polypharmacy | Careful medication usage |
| Lifestyle | Avoid alcohol, unsafe outdoor/indoor activities |
| *Overall weakness/mobility losses | Muscle strengthening/weight-bearing exercises |
| Nutritional deficits | Assess, provide access to desirable nutritional foods |
| Post-operative sarcopenia | Monitor, intervene accordingly |
| Relative cortisol insufficiency | Stress management |
| Vision status | Eyewear reviews/referrals/lighting attributes |
| Vitamin D status | Assure safe levels |
| Sleep challenges | Avoid sleep/hypnotic medications, naps |
| Smoking | Encourage non-smoking |
| Poor understanding of risks/solutions | Health education |
| Weight status | Avoid excess/suboptimal weight |
| Zinc status | Ensure especially post-operatively |
In addition to their annual health reviews, older adults might undergo bone density assessments, and be evaluated periodically for any excess falls or possible fracture risk due to associated progressive muscle mass and strength declines. They might also be monitored for any regression in health status, especially if the older adult is undernourished, and of low body weight, and receiving drugs to counter depression or sleep challenges 20. Where applicable, the ‘at risk’ older adult should also be strongly encouraged to avoid tobacco or excess alcohol usage, and to engage in regular exercise and recommended fall prevention programs, regardless of extent of probable falls risk 20. In addition, referrals to endocrinologists or other osteoporosis specialists should be advanced, if warranted.
In the interim, it appears timely persistent primary prevention efforts are potentially imperative in efforts to minimize the overall burden of hip fractures among older members of society, and especially their oftentimes devastating impacts and need to return to surgery within one year, as well as possible recurrent or subsequent hip fracture occurrences among this population 61, 62, 63, 64, 65, 66, 67. To this end, in addition to more widespread falls prevention programs, prompt emergency, surgery, and comprehensive post operative care, including prevention approaches delivered both at the bedside as well as the home or community are indicated now more than ever, especially among the frail or pre frail 68, prior fallers, and older underweight tall women 89, 90.
Discussion
Although the topic of hip fracture injuries among the older adult population has been studied for several decades in an effort to prevent these oftentimes devastating injuries, a fair percentage of current reports indicate this condition remains a highly prevalent one, as well as a severely debilitating one,if indeed the older adult survives surgery. Especially problematic are multiple negative post operative health outcomes including the risk of secondary hip fractures. However, even if hip fractures as a whole are the most costly forms of fracture occurrences 79, very little progress in averting their incidence prevails. Well designed targeted primary, tertiary as well as secondary preventive efforts are however, likely to offset the risk of an older adult incurring this unwanted debilitating injury and its attendant immense social and personal costs 79.
The possibilities are quite numerous here in our view as conceptualized in Table 1. For example, those older adults with multiple co existing health conditions who appear at greater risk for long term disability in the face of one or more hip fractures may benefit from a protective health promotion program starting in early adulthood as well as comprehensive falls prevention efforts. Moreover, loneliness and depression determinants can be treated as indicated, as can malnutrition, frailty, bone fragility, sleep disturbances, and cognitive challenges that can underpin first as well as second hip fractures. Indeed, as discussed by Jain et al. 50, several current studies have shown older adults with fractures may also present with medical comorbidities such as diabetes, stroke, and hypertension that warrant control where present, as well as weakened muscular and bone systems, because they may otherwise be especially vulnerable to injury and recovery complications, if untreated or ignored.
In this regard, it appears many at risk older adults residing in the community may yet sustain a preventable second hip fracture, if dedicated care resources and efforts to prevent any progressive muscle and bone mass losses are overlooked, along with the risk of frailty, poor balance, and gait disturbances 67, 68, 72. Physical activity, may hold the key here to prevent chronic disease flares, and fall injuries attributable to poor motor control and/or unrelenting depressive feelings.
While the reports reviewed were not all inclusive, it seems safe to say global trends in hip fracture prevalence will persist unless the need for future preventive and intervention approaches is recognized in a timely manner, regardless of country of origin. However the available data indicate little change between 1970 and 2026 in terms of documented second hip fracture occurrences and their severity, although these vary from eight to fifteen percentage points over time. In particular, all reports are largely in agreement that mortality rates are increased in the presence of a second hip fracture, regardless of fracture site. However, a role for malnutrition, social isolation factors, pain, and possible multiple cognitive, muscle and bone mass factors that are potentially amenable to alteration are not well articulated though, or unified, if at all in most studies, regardless of fracture type.
Indeed, the most frequent determinants observed and reported in the literature and highlighted in Table 1 and Figure 1, including poor health status, vision, muscle weakness, and falls injuries are attributes that are possibly somewhat preventable or modifiable 69. In addition, focusing on the role of comorbid conditions, cognitive disorders, subnormal cortisol stress responses 80, as well as the impact of psychotropic drug usage, which again are reported very sporadically, may prove of further benefit in multiple ways. In this respect, recent data have indicated those older adults who sustain subtrochanteric hip fractures as well as those older adults presenting with a high risk profile for subsequent fragility fractures, should probably be selectively monitored for extended periods after any hip fracture surgery 64, 66, 70, possibly for at least five years 71. As well, ensuring their homes are safe and bone building resources are advanced thoughtfully appear strongly indicated 10 alongside routine muscle assessments 72 and limiting excessive drug use, and monitoring postoperative cortisol levels 80.
Figure 1. Schematic representation of possible adverse effects of poorly treated hip fractures on recurrent hip fracture risk among older community dwelling older adults.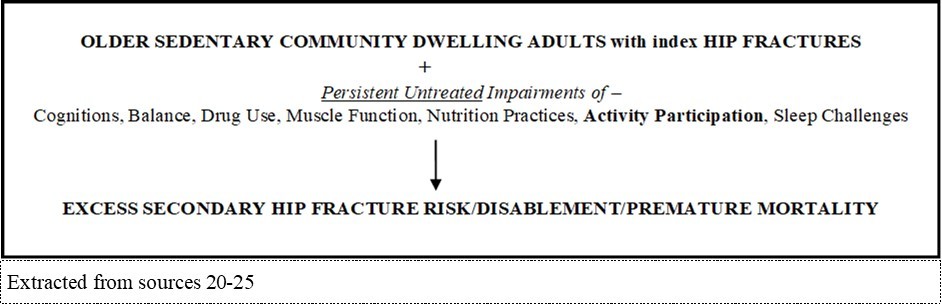
Download figure
Figure 2. Possible hip fracture preventive benefits of physical activity participation
Download figure
In essence, from the outset, it appears, continued vigilance in the realms of primary, secondary and tertiary prevention is needed to help the aging adult to maintain an optimal health status and activity level, along with any ongoing rehabilitation needs presented by a hip fracture incident. Here, one possible mutual goal of paramount importance in the context of averting hip fracture incidents, primary or secondary, is a heightened falls risk consequent to muscle strength losses that negatively impact successful joint protection and gait, and foster a state of post falling vulnerability as outlined in Figure 273, 74, 75. Alternately, because weakness can hasten bone demineralization, as well as diminish protective response across injured as well as uninjured limbs, as well as coverage of the underlying bone, suboptimal related attempts to offset hip fractures at any stage may fail, especially in the face of pre-existing co-morbidities, or having a falls and fragility fracture history 84.
Moreover, it appears a sole reliance on passive strategies in this regard may have little to no benefit on the prevention of one or more hip fractures and falls 81, for example if the older adult is deemed a recurrent faller due to dementia 89, or is consistently exposed to polyphamacology 82, or suffers from untreated osteoporosis 76 or cardiovascular disease 73. In addition the failure to avert muscle atrophy due to sedentary behaviors, may hasten hip fracture occurrences and magnitude in frail vulnerable high age adults 65, 73.
On the other hand, in addition to heightened geriatric care, much needed efforts to minimize the multiple possible burgeoning hip fracture societal costs, public health organizations and personnel can potentially help enormously by encouraging safe forms of physical activity participation and exercises that promote muscle strength, regardless of health status 85, 86, 87, 88. Older adults at risk for frailty, who avoid exercising due to pain and falls fears, and those admitted to and operated on in a hospital setting and exhibiting vitamin D and calcium deficiencies should be targeted as well 75, 76, 84, 86.
Until then, if more is not done in a timely, insightful, and far-reaching committed manner in this regard, the excess suffering currently prevailing among many older adults is likely to escalate accordingly for years to come.
Key conclusions
Despite the limitations of this report and immense gaps in the literature, we believe this overview spanning a 50 year+ time period supports the view that surgery alone for repairing an index hip fracture among older adults, is necessary, but not sufficient to offset future excess debility and mortality rates attributable to subsequent fractures found to occur in sizeable numbers of cases.
In line with the expressed consensus on the gravity of incurring a hip fracture by many, if not all researchers, we conclude:
· This situation may yet be compounded as adults live to higher ages, but with high levels of associated chronic health challenges both physical and emotional.
· In addition, we conclude that until more research prevails to recognize and identify modifiable risk factors and their attenuation, concerted multi pronged carefully construed personalized preventive efforts pre and post index hip fracture surgery while appearing strongly warranted, especially among older adults deemed at risk for frailty or who are already frail, may yet fail.
· Moreover, to avert excess human and fiscal costs among the first and second hip fracture population, we conclude more concentrated health promotion efforts that are part of health maintenance programs in early adulthood, plus carefully construed long term post index fracture targeted multi pronged rehabilitation and follow up assessments are strongly recommended.
· In this regard, we further conclude high risk older adults living alone in the community, especially those with multiple chronic diseases and/or a low bone, muscle, and body mass, plus those living in unsafe housing, or with cognitive challenges should be specifically targeted sooner rather than later.
To achieve success, it appears safe to conclude, regular physical activity participation potentially offers the most beneficial preventive hip fracture path at all stages of aging and is consistent with the documented role of multiple muscle and bone attrition related changes that may fail to avert falls injuries on one occasion, as well as possibly on multiple occasions.
Closing remarks
Among the many related remediable hip fracture risk factors, low physical activity levels appear especially important to counteract its disabling impacts, which includes disability costs, nursing care, rehabilitation care and surgical costs that are predicted to rise by 2050. By contrast, it appears physical activity participation can help to reduce the prevalence and excess disability of hip fractures occurrences and should be strongly encouraged across the spectrum of aging, as well as among ‘high risk’ and/or actual hip fracture populations no matter where they reside.
References
- 1.H K Kjeldgaard, Abrahamsen B, M N Händel, B L Heitmann, H E Meyer et al. (2025) Explaining the declining hip fracture incidence in Denmark 1999-2018. The Hip-IMPACT model. , The European Journal of Public Hlth 35.
- 2.K F Axelsson, Litsne H, N C Harvey, J A Kanis, McCloskey E et al. (2026) Revised Swedish FRAX models and the establishment of age-dependent intervention thresholds. , Osteoporosis International.,Apr 23.
- 3.A C Meyer, Ek S, Drefahl S, Ahlbom A, Hedström M et al. (2021) Trends in hip fracture incidence, recurrence, and survival by education and comorbidity: A Swedish Register-based study. , Epidemiol 32(3), 425-433.
- 4.Nordström P, Bergman J, Ballin M, Nordström A. (2022) Trends in hip fracture incidence, length of hospital stay, and 30-Day mortality in Sweden from 1998-2017: A nationwide cohort study. , Calc Tissue Int 111(1), 21-28.
- 5.Sun W, Dai Z, Lin X, Fang K. (2026) Disease burden attributable to hip fractures in Asian women. , International Journal of Women's Hlth 18, 586201.
- 6.Masionis P, Vaitukaitis G, Masionienė A, Uvarovas V, Šatkauskas I. (2026) Risk factors associated with complications and early mortality of hip fracture surgery in elderly patients. , Medicina (Kaunas, Lithuania) 62(5), 825.
- 7.C F Herbosa, Pettit C, Ganta A, Egol K, Konda S. (2026) The terrible 2s: twice the risk of inpatient complications in 2nd geriatric hip fractures. Hip Int. 11207000251398425.
- 8.Yiğit Ş, Ozkul E, Çevik N, Kaydu A, Yigit A. (2026) The effect of bone minerals density on mortality of elderly patients applying with a proximal fracture of the femur. , Acta Chirurgiae Orthopaedicae Et Traumatologiae Cechoslovaca 93(2), 67-71.
- 9.Zhang C, Feng J, Wang S, Gao P, Xu L et al. (2020) Incidence of and trends in hip fracture among adults in urban China: A nationwide retrospective cohort study. , PLoS Med 17(8), 1003180.
- 10.Qi X, Lu L, Li H, Sun Z, Li Y et al. (2026) Trends, disease burden, and cause patterns of hip fracture among older adults from. to 2023 in mainland , Archives Osteoporos 21(1), 72.
- 11.S R Pekonen, Kopra J, Kröger H, Rikkonen T, Sund R. (2021) Regional and gender-specific analyses give new perspectives for secular trend in hip fracture incidence. , Osteoporos Int 32(9), 1725-1733.
- 12.I L Kyrdalen, B H Strand, Selbæk G, Thingstad P, Ormstad H et al. (2024) Prevalence and future estimates of frailty and pre-frailty in a population-based sample of people 70 years and older in Norway: the HUNT study. Aging Clinical and Experimental Res. 36(1), 188.
- 13.Rapp K, Büchele G, Dreinhöfer K, Bücking B, Becker C et al. (2019) Epidemiology of hip fractures: Systematic literature review of German data and an overview of the international literature. , Z Gerontol 52(1), 10-16.
- 14.K B Lin, N P Yang, Y H Lee, C L, C H Wu. (2018) The incidence and factors of hip fractures and subsequent morbidity in Taiwan: An 11-year population-based cohort study. PLoS One.,13(2), e0192388
- 15.Saleh Y, R A Sulimani, Alomary S, Y I Alnajjar, Vandenput L et al. (2022) Incidence of hip fracture in Saudi Arabia and the development of a FRAX model. , Saudi FRAX Study Group 17(1), 56.
- 16.Y W Zhang, P, Y J Li, G C Dai, M H Chen et al. (2021) Prevalence, characteristics, and associated risk factors of the elderly with hip fractures: A cross-sectional analysis of NHANES 2005-2010. , Clin Intervent Aging 16, 177-185.
- 17.S C Perez, G A Cruz-Priego, Clark P, Ortiz-Barboza A, Johansson H et al. (2026) Epidemiology of hip fractures in Costa Rica and development of country- specific thresholds to estimate fracture risk. , Archives of Osteoporos 21(1), 30.
- 18.J A Cauley, P M Cawthon, K E Peters, S R Cummings, K E Ensrud et al. (2016) C.,et al.,& Osteoporotic Fractures in Men (MrOS). , Study Research Group 31(10), 1810-1819.
- 19.Kjærvik C, J E Gjertsen, Stensland E, Saltyte-Benth J, Soereide O. (2022) Modifiable and non-modifiable risk factors in hip fracture mortality in Norway. , Jt J 104, 884-893.
- 20.Inoue S, Otaka Y, Kawakami M, Kitamura S, Kondo K. (2026) Fall risk and falls count by functional status in patients with hip fracture. , BMC Geriatric. Doi: 10-1186.
- 21.K E Dretakis, E K Dretakis, E F Papakitsou, Psarakis S, Steriopoulos K. (1998) Possible predisposing factors for the second hip fracture. , Calcif Tissue 62(4), 366-369.
- 22.Dolk T. (1989) Influence of treatment factors on the outcome after hip fractures. , Upsala J Med Sci 94(2), 209-221.
- 23.H M Schroder, K, Erlandsen M. (1993) Occurrence and incidence of the second hip fracture. Clin Orthop Rel Res..289:. 166-169.
- 24.Scaglione M, Fabbri L, F Di Rollo, M G Bianchi, Dell'omo D et al. (2013) The second hip fracture in osteoporotic patients: Not only an orthopaedic matter. Clin Cases in Mineral Bone Metab. 10(2), 124-128.
- 25.Yamanashi A, Yamazaki K, Kanamori M, Mochizuki K, Okamoto S et al. (2005) Assessment of risk factors for second hip fractures in Japanese elderly. , Osteoporos Int 16(10), 1239-1246.
- 26.Nymark T, J M Lauritsen, Ovesen O, N D Röck, Jeune B. (2006) Short time-frame from first to second hip fracture in the Funen County Hip Fracture Study. , Osteoporos Int 17(9), 1353-1357.
- 27.Lönnroos E, Kautiainen H, Karppi P, Hartikainen S, Kiviranta I et al. (2007) Incidence of second hip fractures. A population-b ased study. , Osteoporosis Int 18(9), 1279-1285.
- 28.Chen M, Du Y, Tang W, Yu W, Li H et al. (2022) Risk factors of mortality and second fracture after elderly hip fracture surgery in Shanghai. , China. J Bone Mineral Metab 1-9.
- 29.Trevisan C, Bedogni M, Pavan S, Shehu E, Piazzani F et al. (2020) The impact of second hip fracture on rehospitalization and mortality in older adults. , Arch Gerontol Geriatr 90, 104175.
- 30.Guy P, Sobolev B, K J Sheehan, Kuramoto L, K A Lefaivre. (2017) The burden of second hip fractures: Provincial surgical hospitalizations over 15 years. , Can J Surg 60(2), 101-107.
- 31.Leal J, Gray A M, Prieto-Alhambra D, Arden N K, Cooper C et al. (2016) A; REFReSH study group. , Int 27(2), 549-558.
- 32.O S Atik. (2014) Second hip fracture in elderly patients. , Eklem Hastaliklari Ve Cerrahisi 25(3), 125.
- 34.S B Lee, Park Y, D W Kim, J W Kwon, J W Ha et al. (2021) Association between mortality risk and the number, location, and sequence of subsequent fractures in the elderly. , Osteoporos Int 32(2), 233-241.
- 35.Liu S, Zhu Y, Chen W, Sun T, Cheng J et al. (2015) Risk factors for the second contralateral hip fracture in elderly patients: A systematic review and meta-analysis. , Clin Rehabil 29(3), 285-294.
- 36.Egan M, Jaglal S, Byrne K, Wells J, Stolee P. (2008) Factors associated with a second hip fracture: A systematic review. , Clinical Rehabi 22(3), 272-282.
- 37.Mitani S, Shimizu M, Abo M, Hagino H, Kurozawa Y. (2010) Risk factors for second hip fractures among elderly patients. , J Orthop Sci 15(2), 192-197.
- 38.S H Lee, I J Chen, Y H Li, Chiang Fan, Y C et al. (2016) Incidence of second hip fractures and associated mortality in Taiwan: A nationwide population-based study of 95,484 patients during 2006-2010. Acta Orthop Traumatol Turcica. 50(4), 437-442.
- 39.T M Lawrence, Wenn R, C T Boulton, C G Moran. (2010) Age-specific incidence of first and second fractures of the hip. , J Bone Jt Surg 92, 258-261.
- 40.Hagino H, Sawaguchi T, Endo N, Ito Y, Nakano T et al. (2012) The risk of a second hip fracture in patients after their first hip fracture. , Calcified Tissue Int 90(1), 14-21.
- 41.L M Kok, Steenhoven T J van der, R G Nelissen. (2011) A retrospective analysis of bilateral fractures over sixteen years: Localisation and variation in treatment of second hip fractures. , Int Orthop 35(10), 1545-1551.
- 42.Wongtriratanachai P, Chiewchantanakit S, Vaseenon T, Rojanasthien S, Leerapun T. (2015) Second hip fractures at Chiang Mai University Hospital. , J Med Assoc Thailand 98(2), 201-206.
- 43.T K Omsland, Holvik K, H E Meyer, J R Center, Emaus N et al. (2012) Hip fractures in Norway 1999-2008: Time trends in total incidence and second hip fracture rates: A NOREPOS study. , Eur J Epidemiol 27(10), 807-814.
- 44.Bynum J, J E Bell, R V Cantu, Wang Q, C M McDonough et al. (2016) Second fractures among older adults in the year following hip, shoulder, or wrist fracture. , Osteoporosis Int 27(7), 2207-2215.
- 45.H Q Sheikh, F S Hossain, Khan S, Usman M, Kapoor H et al. (2019) Short-term risk factors for a second hip fracture in a UK population. , Eur J Orthop Surg Traumatol 29(5), 1055-1060.
- 46.Downey C, Flannery S, Murphy B, Daly T, Conway S et al. (2022) A multi-site review of second hip fractures across 6 Dublin teaching hospitals. , Irish J Med Sci 759-764.
- 47.Downey C, Flannery S, Wahab Abd, H E, Askin D et al. (2020) The patient's second hip fracture - One in ten. , Irish Med J 113(6), 93.
- 48.Helynen N, Rantanen L, Lehenkari P, Valkealahti M. (2022) Predisposing factors for a second fragile hip fracture in a population of 1130 patients with hip fractures, treated at Oulu University Hospital in 2013-2016: A retrospective study. Arch Orthop Trauma Surg.Doi:. 10-1007.
- 49.Zidrou C, A V Vasiliadis, Rizou S, Beletsiotis A. (2022) Second hip fracture in older adults: incidence and risk factors. , Eur J Orthop SurgTtraumatol.Doi: 10-1007.
- 50.Solou K, Tyllianakis M, Kouzelis A, Lakoumentas J, Panagopoulos A. (2022) Morbidity and mortality after second hip fracture with and without nursing care program. , Cureus 14(3), 23373.
- 51.Fujita T, Takegami Y, Ando K, Sakai Y, Nakashima H et al. (2022) Risk factors for second hip fracture in elderly patients: an age, sex, and fracture type matched case–control study. , Eur 32(3), 437-442.
- 52.Larrainzar-Garijo R, Díez-Pérez A, Fernández-Tormos E, Prieto-Alhambra D. (2021) Risk factors for a second nonsimultaneous hip fracture in a prospective cohort study. Arch Orthop Trauma Surg.Doi:. 10-1007.
- 53.Wang L, Yin L, Yang M, Ge Y, Liu Y et al. (2022) Muscle density is an independent risk factor of second hip fracture: A prospective cohort study. , J Cachexia, Sarcopenia Muscle 13(3), 1927-1937.
- 54.M K Javaid, Mohsin Z, Johansen A, Gregson C, Pinedo-Villanueva R. (2022) Subsequent hip fractures in patients identified by a Fracture Liaison Service (FLS) in England and Wales: linkage of the national FLS and Hip Fracture databases.
- 55.Schemitsch E, J D Adachi, J P Brown, J E Tarride, Burke N et al. (2022) Hip fracture predicts subsequent hip fracture: A retrospective observational study to support a call to early hip fracture prevention efforts in post-fracture patients. , Osteoporos Int 33(1), 113-122.
- 56.A C Meyer, Ek S, Drefahl S, Ahlbom A, Hedström M et al. (2021) Trends in hip fracture incidence, recurrence, and survival by education and comorbidity: A Swedish Register-based Study. Epidemiology. , (Cambridge, Mass.) 32(3), 425-433.
- 57.R B Conley, Adib G, R A Adler, K E Åkesson, I M Alexander et al. (2020) Secondary fracture prevention: Consensus clinical recommendations from a multistakeholder coalition. , J Bone Min Res 35(1), 36-52.
- 58.Inoue T, Maeda K, Nagano A, Shimizu A, Ueshima J et al. (2020) Undernutrition, sarcopenia, and frailty in fragility hip fracture: advanced strategies for improving clinical outcomes. , Nutrients 12(12), 3743.
- 59.Min K, Beom J, B R Kim, S Y Lee, G J Lee et al. (2021) Clinical practice guideline for postoperative rehabilitation in older patients with hip fractures. , Ann Rehabil Med 45(3), 225-259.
- 60.J I Yoo, J T Kim, C H Park, Cha Y. (2022) Diagnosis and management of sarcopenia after hip fracture surgery: Current concept review. , Hip & Pelvis 34(1), 1-9.
- 61.Ren J, Liu M, Wang B, Bai C, Yang K et al. (2026) Secondary fracture risk after hip fracture in older patients: an updated sex-specific systematic review and meta analysis with GRADE and PAF assessment. , Osteoporosis 10-1007.
- 62.Patel R, Judge A, Johansen A, M K Javaid, Marques E M R et al. (2026) Reoperation in the year following a hip fracture: A nationwide cohort study in England. , The Bone & Joint J 108, 698-706.
- 63.Blattner A, Sabath F, Röttinger T, Lisitano L, Mayr E et al. (2026) Second contralateral hip fractures reduce survival, mobility and daily activity : a matched pair analysis. , Archives of Orthopaedic and Trauma Surg 146(1), 177.
- 64.Ho A, S H Wong. (2020) Second hip fracture in Hong Kong - Incidence, demographics, and mortality. , Osteoporos Sarcopenia 6(2), 71-74.
- 65.Llopis‐Cardona F, Armero C, Hurtado I, García‐Sempere A, Peiró S et al. (2022) Incidence of subsequent hip fracture and mortality in elderly patients: A multistate population‐based cohort study in Eastern Spain. , J Bone Min Res 37(6), 1200-1208.
- 66.H J Aguado, Castillón-Bernal P, P S Ventura-Wichner, M C Cervera-Díaz, Abarca-Vegas J et al. (2022) Impact of subtrochanteric fractures in the geriatric population: better pre-fracture condition but poorer outcome than pertrochanteric fractures: Evidence from the Spanish Hip Fracture Registry. , RNFC Working Group 23(1), 17.
- 67.Ma Y, Wang A, Lou Y, Peng D, Jiang Z et al. (2022) Effects of frailty on outcomes following surgery among patients with hip fractures: A systematic review and meta-analysis. , Frontiers Med 9, 829762.
- 68.K S Miranda, L R Calderón, Piedra S, Ochoa-Andrade M. (2026) Sociodemographic determinants of intertrochanteric hip fractures in older adults: evidence from a six-year retrospective study in an Ecuadorian hospital. Frontiers in surgery. 13, 1732009-10.
- 69.A J Vochteloo, Burg Borger van der, L B, M A Röling, Leeuwen D H van et al. (2012) Contralateral hip fractures and other osteoporosis-related fractures in hip fracture patients: Incidence and risk factors. An observational cohort study of 1,229 patients. , Arch Orthop Trauma Surg 132(8), 1191-1197.
- 70.S N Morin, Yan L, L M, W D Leslie. (2021) Long-term risk of subsequent major osteoporotic fracture and hip fracture in men and women: A population-based observational study with a 25-year follow-up. , Osteoporos Int 32(12), 2525-2532.
- 71.S H Woo, K S Park, I S Choi, Y S Ahn, D M Jeong et al. (2020) Sequential bilateral hip fractures in elderly patients. , Hip & Pelvis 32(2), 99-104.
- 72.Nolan P, Tiedt L, Ellanti P, McCarthy T, Hogan N. (2020) Incidence of non-simultaneous contralateral second hip fractures: A single-center Irish Study. , Cureus 12(10), 11154.
- 73.S H, K C Huang, Y H Tsai, T Y Yang, M S Lee et al. (2014) Risk analysis for second hip fracture in patients after hip fracture surgery: A nationwide population-based study. , J Am Med Dir Assoc 15(10), 725-731.
- 74.Mazzucchelli R, Pérez-Fernández E, Crespí N, García-Vadillo A, Caravaca Rodriguez et al. (2018) Second hip fracture: Incidence, trends, and predictors. , Calc Tissue Int 102(6), 619-626.
- 75.Chen J, Xie F, Ke M, Zhuo H, Li X et al. (2026) Dynamic frailty trajectories, multidimensional resilience, and risk of incident hip fracture: A prospective cohort study with competing risk analysis. , Archives of Gerontology and Geriatric 147, 106265.
- 76.Ali A, Senthinathan A, Rashidian L, Y Q Bai, W P et al. (2026) The association between hospital harms and 1-year mortality following a hip fracture in Ontario, Canada: A cohort study. , Journal of the American Geriatrics Soc.Doi: 10-1111.
- 77.Tao X, Guo F, Wang L, Zhao H. (2026) Analysis of latent profiles and influencing factors of fall risk perception in elderly patients with hip fracture. , BMC Geriatric 26(1), 586.
- 78.Unno H, Hasegawa T, Sato M, Kobayashi G, Tone S et al. (2026) Association between perioperative zinc supplementation and recovery of walking ability after hip fracture surgery: a propensity score-matched study. , InternationalOrthopaedic.Doi: 10-1007.
- 79.M P Høiberg, Gram J, Hermann P, Brixen K, Haugeberg G. (2014) The incidence of hip fractures. in Norway -accuracy of the national Norwegian patient registry.BMC Musculoskelet Disord.15 372.
- 80.M, L E Streck, B J, S C Herath, C K Audretsch et al. (2026) The cortisol stress response following surgery for proximal femur fractures in geriatric patients - a prospective pilot study. , Frontiers in Endocrinol 17, 1820534.
- 81.Massé O, C M Mercurio, Dupuis S, Sahwi Al, Arruda M et al. (2026) Calcium, vitamin D, or combined supplementation to prevent fractures and falls: systematic review and meta-analysis. , BMJ (Clinical Research Education J 393, 088050.
- 82.García-Tercero E, Valcuende-Rosique A, Valcuende-Rosique A, Rubio D A V, A N Bono et al. (2026) Real-world evidence of the impact of polypharmacy on mortality and recovery after hip fracture in elderly patients. Scientific Rep. 10-1038.
- 83.Hossain R, Laddu D, C J, K E Ensrud, J A Cauley et al. (2026) The association between 10-year cardiovascular risk and fracture incidence in postmenopausal women: A prospective analysis from the Women's Health Initiative. , Lancet Regional Health Am 57, 101440.
- 84.Lv W, Lin J, Lin K, Wen X, Lin Q et al. (2026) Vitamin D status and site-specific fracture pattern associations in older adults with fragility fractures: a cross-sectional analysis of 2543 patients. , Frontiers in Nutr 13, 1810545.
- 85.Nagamine T. (2026) The contralateral muscle reserve: rethinking post-operative risk stratification and discharge trajectories in acute hip fracture care. , Geriatrics & Gerontology Int 26(5), 70546.
- 86.Unnanuntana A, Kuptniratsaikul V, Srinonprasert V, Charatcharoenwitthaya N, Kulachote N et al. (2023) A multidisciplinary approach to post-operative fragility hip fracture care in Thailand - a narrative review. , Injury 54(11), 111039.
- 87.Yin H, Qin C, Tang Q, Wu G, Diao H. (2026) Postoperative sarcopenia in older patients with hip fractures: incidence and associated risk factors in a retrospective cohort study. , Frontiers in Med 13, 1766120.
- 88.R Z Xie, Zhao N, X S Li, F Z Li, W Q Zhao et al. (2025) Aging-related muscle mass decline in hip fracture patients across age groups.Ann Med.,57(1). 2578427.
- 89.Yuan Y, Zhang M, P Y Li, Wang W, Y N Lu et al. (2025) Subsequent fracture risk after hip fracture surgery in China: a three-year retrospective cohort study. , BMC Geriatric 26(1), 210.
- 90.Sjölander M, Alvunger L, Eggertsen R, Lindgren A, Mölstad U et al. (2026) Reduced risk of recurrent fragility fractures after a primary care-based fracture prevention intervention: A 20-year non-randomized controlled follow-up study in women aged 70-100. , Scandinavian Journal of Primary Health Care 44(1), 1-16.