
Pleomorphic Adenoma of The Nasal Septum
Abstract
Pleomorphic adenomas are uncommon tumors of the nasal cavity. They arise from minor salivary glands, and usually originate from the nasal septum. The tumors are more common in middle-aged females. We present a series of 8 cases of intranasal pleomorphic adenomas. Seven of these tumors originated from the nasal septum, and only one of them originated from the lateral nasal wall. Histopathologic examination of the tumors showed that these tumors have higher epithelial and lower stromal components compared to pleomorphic adenomas of major salivary glands. Endoscopic resection was performed in all cases and the patients were followed up for one year. No recurrences or complications were observed in this series. Endoscopic resection is recommended as the treatment of choice because of its proven efficacy and low morbidity.
Author Contributions
Academic Editor: Ioannis Chatzistefanou, Aristotle University of Thessaloniki (A.U.Th), Department of Maxillofacial Surgery, G. Papanikolaou General Hospital
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2014 Samy Elwany, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Salivary gland neoplasms are uncommon and make up less than 5% of all head and neck neoplasms. Pleomorphic adenoma is the most common benign salivary gland tumor. Parotid gland tumors constitute 60% of all pleomorphic adenomas, while minor salivary glands constitute only 8% of them1. Pleomorphic adenomas of minor salivary glands may develop in any site where the minor salivary glands exist2. Rare cases have been reported in the nasal cavity, nasopharynx, oropharynx, and larynx. Intranasal pleomorphic adenomas are rare, slow growing tumors3. These tumors are frequently misdiagnosed because they are usually highly cellular and have few myxoid stroma,,4,5,6In this paper, we present a case series of pleomorphic adenomas of the nasal cavity and discuss the literature on this uncommon tumor. In addition, we discuss relevant issues about the pathology, diagnosis, and management of the tumor.
Patients and Methods
The study included 8 patients (5 females and 3 males) with the diagnosis of nasal pleomorphic adenoma during the period from January 2003 to December 2012. Endoscopic examination was done, and radiological studies included computed tomography (MDCT) with ultra-thin 1mm cuts and multiplanar reconstruction, and magnetic resonance imaging (MRI).
Complete endoscopic excision of the mass, including the surrounding mucosa / mucoperichondrium, was performed in all cases.
The patients were followed up weekly for the first month and then every 2 weeks until complete healing has occurred. Complete healing usually took place after 8 - 12 weeks. All cases were then re-examined one year postoperatively.
Informed consents from all the patients was taken prior to surgery after they were fully informed about the details of the surgical procedure. The Institutional Review Board (IRB) approved the study.
Results
The study series included 8 patients with nasal pleomorphic adenoma (Table 1). The series included 5 females and 3 males, with a mean age of 38.8 years (32 -47 years). All patients presented with unilateral nasal obstruction Three of them presented with external nasal swelling, and two of them presented with mild epistaxis.
Table 1. Characteristics of the patients| Patients | Age (years) | Sex | Main Symptoms | Site of origin |
| 1 | 34 | Female | Nasal Obstruction, Nasal Discharge | Nasal Septum |
| 2 | 41 | Male | Nasal Obstruction | Nasal Septum |
| 3 | 36 | Female | Nasal Obstruction, Nasal Discharge, External Swelling | Nasal Septum |
| 4 | 50 | Female | Nasal Obstruction, Epistaxis | Nasal Septum and Floor of the nose |
| 5 | 47 | Male | Nasal Obstruction, External Swelling | Nasal Septum |
| 6 | 32 | Female | Nasal Obstruction | Nasal Septum |
| 7 | 39 | Female | Nasal Obstruction, Nasal Discharge, Epistaxis | Lateral nasal wall |
| 8 | 44 | Male | Nasal Obstruction, External Swelling | Nasal Septum |
Endoscopic examination, in all cases, revealed a well-defined moderately firm mass that did not bleed on gentle touch (Figure 1a). CT scans showed a well-defined soft tissue mass with a smooth border. The mass expanded the external nose in 3 cases (Figure 1b).
In all cases, the mass was excised endoscopically under general hypotensive anesthesia. During surgery, the tumor was found to be attached to the nasal septum in 7 cases and to the lateral nasal wall in front of the middle turbinate in a single case .The tumor was excised together with the underlying mucosa / mucoperichondrium leaving a bare area corresponding to the size of the tumor (Figure 1c). The postoperative course was uneventful and no complications were encountered. The bare areas healed completely within few weeks (Figure 1d).
The final histopathologic result for the tumor, in all cases, was pleomorphic adenoma, and the resection margin was tumor free. The tumor was composed of abundant polygonal epithelial and spindle-shaped myoepithelial elements in a myxofibrous stroma (Figure 2).
Figure 1.a-Endoscopic view of the adenoma. S: Septum, L: Lateral wall, b-Coronal CT scan showing the adenoma (arrow), c-The excised adenoma, d-Complete healing of the septum (S).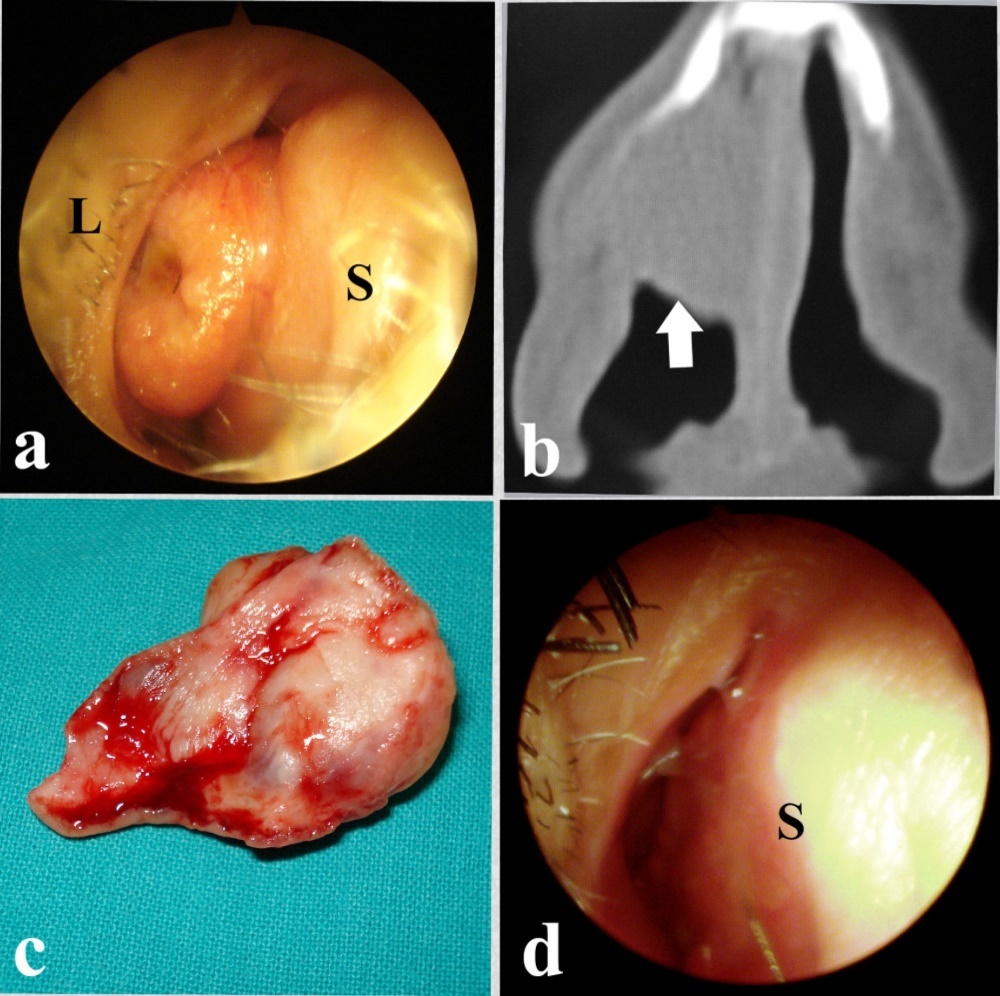
Figure 2.a-Histopathologic section showing a benign non-encapsulated tumor under respiratory epithelial lining b-The tumor is composed of polygonal epithelial and spindle-shaped myoepithelial elements in a myxofibrous stroma (H&E, x200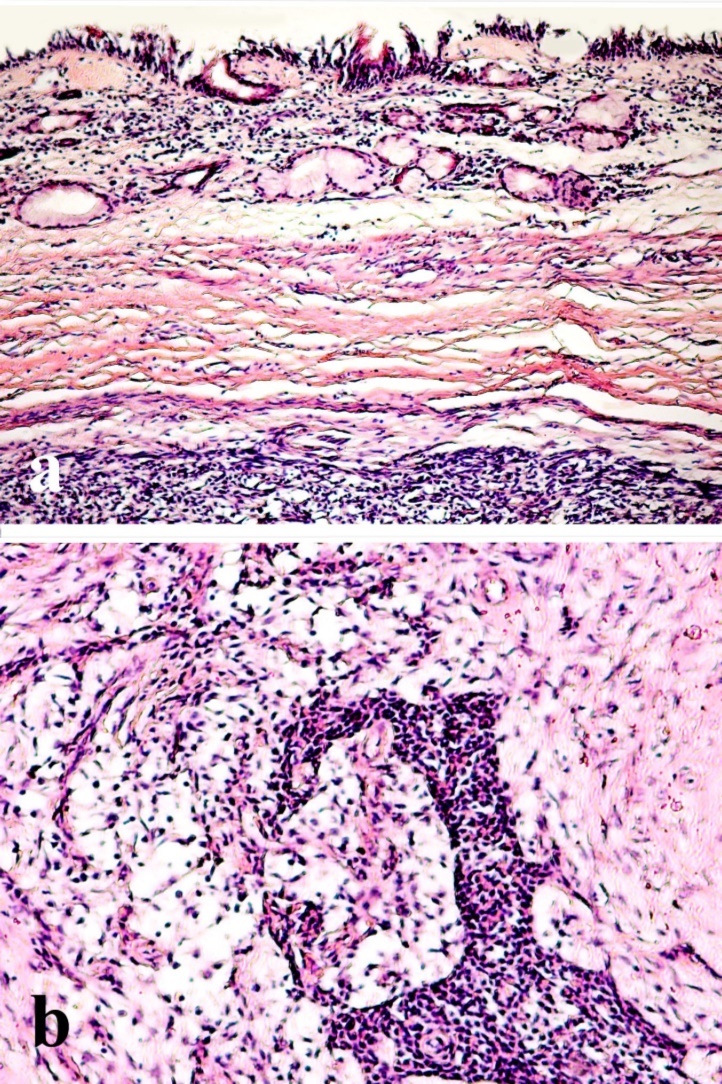
Discussion
Pleomorphic adenomas are the most common tumor of the major salivary glands, but are unusual in the respiratory tract. Rare cases have been reported in the nasal cavity, paranasal sinuses, pharynx, and larynx. Batsakis stated that within the upper respiratory tract, the most favored site of origin is the nasal cavity, followed by the maxillary sinus and nasopharynx.1 Fewer than 20% of the intranasal pleomorphic adenomas were noted to have arisen from he lateral nasal wall7, 8 with the rest originating from the nasal septum.9, 10, 11, 12 The majority of the tumors are noted in the third to sixth decades of life, and the patients typically present with the complaint of unilateral nasal obstruction. Other less frequent complaints include epistaxis, external nasal swelling, and mucopurulent discharge.
Diagnosis of intranasal pleomorphic adenomas mainly relies on pathologic examination. Pleomorphic adenomas are characterized by epithelial tissue mixed with mucoid and myxoid elements. However in nasal pleomorphic adenomas, myoepithelial cellularity is increased compared with major salivary gland tumors. This may cause difficulty in its histopathologic diagnosis as pointed to by Compagno and Wong5as well as Shih-Hung.13Haberman and Stanely14reported a case of a nasal pleomorphic adenoma misdiagnosed as adenoid cystic carcinoma on the basis of tissue biopsy. Many authors have speculated the pathogenesis of these tumors. It was suggested that nasal pleomorphic adenomas originate from the remnants of vomeronasal (Jacobson’s) organ. However, these adenomas may arise from the lateral nasal wall, where no such organ exists. Evan and Cruickshank15contradicted the previous theory and suggested that these tumors are entirely epithelial tumors that arise in fully developed gland tissue. Malignant transformations and distant metastasis of these tumors are uncommon.16 However, Freeman et al17reported a case of carcinoma ex-pleomorphic adenoma, and Cho et al18reported another 2 cases. These reports highlight the importance of careful histopathologic examination of the specimens.
The treatment of intranasal pleomorphic adenoma involves surgical excision with clear margins. Various approaches have been advocated. Surgical approaches include endonasal endoscopic resection, lateral rhinotomy, and midfacial degloving. Follow up of the patients is strongly recommended since recurrence rates ranging from 2.4% to 7.5% have been previously reported.19 No recurrences were observed in our series. Krolls and Boyce suggested the histologic characteristic most frequently associated with recurrent pleomorphic adenomas was the myxoid stroma, which might easily spills into the surgical field.20 Compagno and Wong attributed the low recurrence rate of intranasal pleomorphic adenomas to its high cellularity and little myxoid stroma.5
Analysis of the results of the present series that endoscopic excision is an effective, reliable, and safe procedure for resection of intranasal pleomorphic adenomas with minimal morbidity, no facial scars, and low rates of recurrence. The approach is equally suitable for both adenomas of the nasal septum as well as adenomas arising from the lateral nasal wall.
In conclusion, pleomorphic adenomas are uncommon tumors of the nasal cavity. They arise from minor salivary glands, and usually originate from the nasal septum. The tumors are more common in middle-aged females. Histologically, they have higher epithelial and lower stromal components compared to pleomorphic adenomas of major salivary glands. Endoscopic resection is the treatment of choice because of its proven efficacy and low morbidity.
References
- 1.Batsakis J W. (1979) Tumors of the Head and Neck : Clinical and Pathological considerations. , Baltimore; Williams,Wilkins: 636-637.
- 2.Baglam T, Durucu C, Cevik C, Kemal B, Oz A et al. (2011) Giant pleomorphic adenoma of the nasal septum. Indian J Otolaryngol Head Neck Surg. 63(4), 393-395.
- 3.Baron S, Koka V, P El Charter, Cucherousset J, Paoli C. (2014) Pleomorphic adenoma of the nasal septum. Eur Ann Otolrhinolaryngol Heas neck Dis. 131(2), 139-141.
- 4.Kuo Y L, Tu T Y, Chang C F, Li W Y, Chang S Y et al. (2011) Extra-major salivary gland pleomorphic adenoma of the head and neck: a 10-year experience and review of the literature.Eur. , Arch Otorhinolaryngol.2011Jul;268 7, 1035-40.
- 5.Compagno J, Wong R T. (1977) Intranasal mixed tumors (pleomorohic adenomas). , Am J Clin Pathol 68, 213-218.
- 6.Kohlberg G D, Scognamiglio T, Reisacher W. (2013) pleomorphic adenoma of the naal septum. , JAMA otolaryngol Head Neck Surg 139(4), 427-8.
- 7.Olajida T G, Alaabi B S, Badmos B K, Bello O T. (2009) Pleomorphic adenoma of the lateral nasal wall- a case report. , Niger Postgrad Med J 16(3), 227-9.
- 8.Sciandra D, Dispenza F, Porcasi R, Kulamarva G, Saraniti C. (2008) Acta Olaryngol Ital. 28(3), 130-3.
- 9.Vallejo Valdezate LA, Menéndez Argüelles ME, Rodríguez Evangelista C, Alonso alonso A, Herrero Laso JL et al. (1994) Adenoma pleomorphic (mixed tumor) in the nasal septum. An Otorrinolaringol Ibero Am. 21(3), 265-73.
- 10.Jackson L E, Rosenberg S L. (2002) Pleomorphic adenoma of the lateral nasal wall. Otolaryngol Head Neck Surg2002;. 127, 474-476.
- 11.Kumar S S, Reddy P S, Prabhakar G. (2004) Pleomorphic adenoma of the nasal septum--a case report. , Indian J Pathol Microbiol.2004Jul; 47(3), 397-8.
- 12.Urbaniec P, Namysłowski G, Lange D, Urbaniec N. (2005) Pleomorphic adenoma of the nasal septum. Otolaryngol Pol. 59(3), 425-7.
- 13.Shih-Hung L, Shih-Hung H, Yen-Liang C. (2005) Pleomorphic adenoma of the nasal septum. Tzu Chi Med J. 17, 47-49.
- 14.Haberman R S, Stanely D E. (1989) Pleomorphic adenoma of nasal septum. Otolaryngol Head Neck Surg. 100, 287-296.
- 15.Evan R W, Cruickshank A H. (1970) Epithelial tumors of the salivary glands. Major problems in pathology. , Philadelphia, PA:WB Saunders Co 167.
- 16.Kamal S A. (1984) Pleomorphic adenoma of the nose: A clinical case and historical review. J Laryngol Otol. 98, 917-923.
- 17.Freeman S B, Kennedy K S, Parkar G S, Tatum S A.Metastasizing pleomorphic adenoma of the nasal septum. Arch Otolaryngol Head Neck Surg 1990;116:. 1331-1333.
- 18.Cho K J, El-Naggar A K, Mahanupab P, Luna M A, Batsakis J G et al.ex-pleomorphic adenoma of the nasal cavity. , J Laryngol Otol1995; 109, 677-679.
Cited by (3)
- 1.Alsaleh Saad, Alharbi Talal, 2024, Pleomorphic adenoma of the nasal septum: A case report, International Journal of Surgery Case Reports, 115(), 109229, 10.1016/j.ijscr.2024.109229
- 2.Aryal Gyan Raj, Shrestha Nischal, Basnet Meenakshi, Shrestha Oshan, Sharma Pratikshya, 2023, Pleomorphic adenoma of nasal septum, an unusual site: a case report from Nepal, Oxford Medical Case Reports, 2023(1), 10.1093/omcr/omac152
- 3.Marlapudi Sudheer Kumar, Bishnoi Tapasya, Sahu PK, kumar Praveen, 2023, Common Tumor in an uncommon location: Pleomorphic Adenoma of nasal cavity – a case Report, Indian Journal of Otolaryngology and Head & Neck Surgery, 75(S1), 947, 10.1007/s12070-022-03446-x