Abstract
Pituitary abscess is extremely rare and often misdiagnosed as pituitary tumor pre-operatively.
We document a case of a 64-year-old lady presented to the outpatient department with complaints of headache and blurring vision of right eye for one month. Based on preliminary investigations, a clinical diagnosis of pituitary adenoma was made and the pituitary gland was surgically excised. Histopathological examination showed Actinomyces infection. This case has been documented due to the extremely rare involvement of the pituitary gland by actinomyces infection. Pituitary abscess is a rare pathology, but it must be considered during evaluating sellar masses, since its prognosis depends on surgical drainage and on the use of specific antibiotics. We report, to our knowledge, the fourth case of Actinomyces israelii infection of the pituitary region.
Author Contributions
Academic Editor: Suraj Konnath George, MD Anderson Cancer Center
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2015 Burcu Yapar, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Sellar masses, constitute a significant portion of intracranial tumors. In the differential diagnosis of sellar lesions; tumors, metastatic tumors, cysts, malformations, inflammatory and vascular events should be present. Inflammatory lesions of the pituitary gland include lymphocytic hypophysitis, pituitary abscesss and granulomatous inflammation. Pituitary abscesss is extremely rare and often misdiagnosed as pituitary tumor pre-operatively. In this report, we present a case of pituitary actinomyces infection, and the clinicopathological and radiologic characteristics are discussed.
Case Report
A 64-year-old lady presented to the outpatient department with complaints of headache and right eye blurring of vision for one month. Neurological examination revealed that bitemporal hemianopsia and impairment of visual acuity. Findings from fundus examination were within normal limits. Rest of the brain appeared unremarkable. Endocrine evaluation was normal. Results of renal function tests, liver function tests and haemogram test were within normal limits. A clinical diagnosis of non-secretory pituitary adenoma was made. Magnetic resonance imaging showed a well-circumscribed contrast-enhancing lesion in the sella (Figure 1, Figure 2). The patient underwent an endoscopic endonasal/transsfenoidal surgery in the supine position and total lesion resection was peformed. Intraoperatively, the lesion was found to be yellow colour, soft and avascular and it was removed totally until the sella turcica was visualized (Figure 3).In histopathologic examination septate hyphae were observed between inflammatory cells, Grocott staining is positive, but acid-fast stain for acid-fast bacilli (AFB) was negative. Histopathological findings suggest that infection of Actinomyces (Figure 4, Figure 5). We performed to patient consulted by patients to infectious diseases clinic. Patients underwent intravenous 6x2 gr ampicillin for four weeks.Then oral 4X500 mg amoxicillin treatment is planned a for at least 6 months. Patient did not have any deficits in the next six months.
Figure 1.White arrow shows on sagittal section of MRI that a well-circumscribed contrast-enhancing lesion in the sella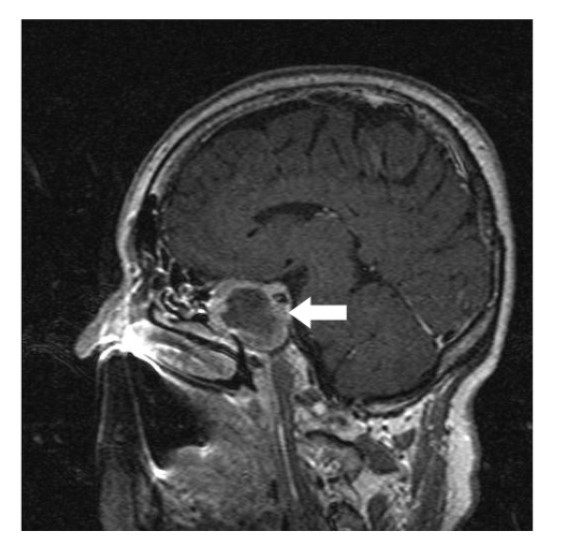
Figure 2.White arrow shows on coronal section of MRI that a well-circumscribed contrast-enhancing lesion in the sella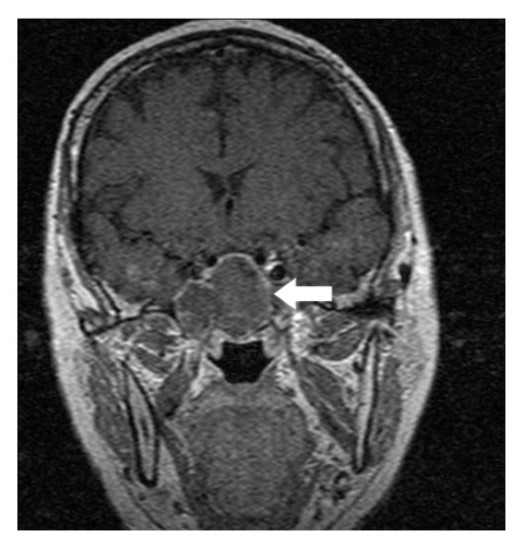
Figure 3.White arrow shows in intraoperative image that the lesion was found as a yellow colour, soft and avascular shape
Figure 4.Light Green PAS stain with filamentous branching bacteria at 10x magnification
Figure 5.Grocott stain with filamentous branching bacteria at 10x magnification
Discussion
Pituitary abscesss is most often of bacterial origin 1. As causative microorganisms, a wide spectrum of agents including gram positive cocci (50% of cases), gram negative bacilli, fungi, and amoebae had been described in the literatüre 2. Spread of infection may be by hematogenous spread, contiguous spread from paranasal sinuses, osteomyelitis or by contaminated cerebrospinal fluid fistula 3.
Actinomycosis caused by the anaerobic gram-positive bacteria the genus Actinomyces. The infection can cause a purulent abscessses and microscopic observations of sulfur granules is characteristic.
Preoperative diagnosis of pituitary abcess is difficult because the presenting symptoms in these patients are similar to that in patients with pituitary adenomas 4. The most common symptoms are headache, vision disturbances and endocrinological abnormalities 5. Magnetic resonance imaging is the best imaging modality for sellar abscess and the features include a hypo- or iso-intense sellar mass on T1-weighted sequences and a hypointense mass on T2-weighted sequences pituitary abscesses may be divided into primary and secondary types. Primary pituitary abscesses occur within a previously healthy gland, while secondary abscesses arise within an existing lesion, such as an adenoma, craniopharyngioma, or Rathke's cleft cyst. Secondary abscesses share radiologic characteristics with the lesions from which they arise. The typical primary pituitary abscess gives the same or slightly lower signal than brain on T1-weighted images, and could be mistaken for a solid mass or presumed to represent a pituitary adenoma. Contrast-enhanced images are useful, demonstrating absence of central enhancement, suggesting a fluid or necrotic center 6.Actinomyces brain abscess is usually diagnosed based on the contrast enhancement on the periphery as in this case.Also MRI spectroscopy findings are the described in actinomyces infection 7, 8.
In order to isolate actinomyces species from clinical specimens need anaerobic processing and provision for a long time for this reason some paints such as gram staining and Grocott filamentous sulfur granules and silver staining are more preferred according to culture for diagnosis 9. Acid-fast stainig not useful in differentiation of actinomyces species from nocardiosis 10.
Actinomyces spp quite sensitive to betalaktam antibiotics. Parenteral and long-term oral Penislin G and amoxicillin therapy is the preferred treatment options 9. Optimal treatment of sellar abscess is transsphenoidal surgery combined with antibacterial therapy.
Conclusion
In conclusion, actinomyces sellar abscess should be considered in the differential diagnosis of a pituitary mass. The correct diagnosis of sellar actinomycosis can only be achieved by histopathological examination of tissue obtained at surgery. The optimal treatment is a combination of surgical resection and appropriate antibacterial therapy.
References
- 1.Vates G E, Berger M S, Wilson C B. (2001) Diagnosis and management of pituitary abscess: A review of twenty-four cases. , J Neurosurg 95, 233-241.
- 2.Altas M, Serefhan A, Silav G, Cerci A, Coskun K K et al. (2013) Diagnosis and management of pituitary abscess: a case series and review of the literature. , Turk Neurosurg 23, 611-616.
- 3.Hoenigl M, Krause R. (2013) Antifungal therapy of aspergillosis of the central nervous system and aspergillus endophthalmitis. Curr Pharm Des. 19, 3648-3668.
- 4.Liu J, You C, Tang J, Chen L. (2013) Fungal pituitary abscess: Case report and review of the literature. , Neurology India 61, 210-212.
- 5.Hao L, Jing C, Bowen C, Min H, Chao Y. (2008) Aspergillus sellar abscess: Case report and review of the literature. , Neurol India 56, 186-188.
- 6.Wolansky L J, Gallagher J D, Heary R F, Malantic G P, Dasmahapatra A et al. (1997) MRI of pituitary abscess: two cases and review of the literature. 39, 499-503.
- 7.Akhaddar A, Elouennass M, Baallal H, Boucetta M. (2010) Focal intracranial infections due to Actinomyces species in immunocompetent patients: diagnostic and therapeutic challenges. , World Neurosurg 74, 346-350.
- 8.Wang S, Wolf R L, Woo J H, Wang J, O'Rourke D M et al. (2006) Actinomycotic brain infection: registered diffusion, perfusion MR imaging and MR spectroscopy. , Neuroradiology 48, 346-350.