
Fear of Falls and Frailty: Cause or Consequence or Both?
Abstract
Background
Many older adults are vulnerable to becoming frail. They are also often at risk for falling and serious injuries and poor health outcomes.
Aim
This exploratory review examines the correlates of frailty, and fear of falling and their association insofar as older adults wellbeing may be jeopardized.
Methods and Procedures
Articles extracted from major electronic data bases that addressed the current topic of interest were used. Key findings regarding the syndromes of frailty and fear of falling were duly downloaded, analyzed and summarized in narrative form.
Results
A high proportion of older adults can be expected to exhibit frailty or become frail as they age. Many too are at risk for falls and fear of future falls, regardless of frailty status. A persistent fear of falls may however, heighten frailty risk or manifestations if not duly addressed in a timely manner.
Conclusion
Prompt comprehensive assessment of at risk older adults, as well as the frail and pre frail older adult, plus those who have fallen may avert serious injury and long term disability plus excess frailty and its deleterious impacts this syndrome has on aging older adults as well as societies.
Author Contributions
Copyright © 2021 Ray Marks
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Aging, a generally accepted biological phenomenon implicating an inevitable declining state of organ and tissue homeostasis is frequently associated with a variety of chronic health conditions, anxiety, depression, various fears, the use of multiple pharmaceutical drugs, nutritional challenges, and multiple physical limitations. Also often associated with various degrees of frailty or a tendency to become frail, this state of increased vulnerability to stress is a potentially preventable critical aging intermediate found to markedly increase the extent of age-associated physical, cognitive, and psychosocial challenges, as well as accelerating overall declines in well being 1, 2. However, even though frailty is a condition expected to increase in prevalence in future years 3, and may predict dementia 2, the possible determinants of frailty attributable to factors other than age and nutrition, such as a high degree of cognitive challenges including the fear of falling-or a lack of confidence in one’s ability to safely undertake active mobility movements, which may heighten frailty, are not well articulated in the mainstream literature. This is despite the possibility that fears evoked by the experience or envisioned experience of falling may represent an important albeit overlooked frailty mediator, and one that is potentially preventable or amenable to modification and to thereby potentially mitigating a variety of cumulative adverse frailty consequences, as well as its onset and exacerbation among older vulnerable adults.
Given the growing need for health providers and others to assist older adults to avoid preventable illnesses or disability states, as well as an excess aging burden and low life quality, and to enable them to age more successfully than not, it appears there may indeed be some merit to examining those factors other than mainstream frailty determinants, as well as falls determinants that may lead to actual fears-a pervasive and serious problem among the elderly 4 associated with a decreased ability to function physically, decreased mobility, muscle weakness, gait disturbances, falls, and a resultant vulnerability to a heightened frailty state 5. In particular, and in light of the severe impact of frailty on all the aforementioned factors, more knowledge in this regard not only appears warranted, but could arguably help to mitigate the rate and degree of downward spiraling of the older adults’ health as well as their frailty status- and in turn, may have immense health implications for both the aging adult, as well as society.
In this regard, this mini review elected to selectively focus on establishing if there is some evidence to support the view that fear of falling can independently or collectively along with other aging features foster frailty, which in turn can predictably engender a high rate of falling related fears and significant injuries and adverse health outcomes.
Indeed, this idea, although possibly not novel, may yet prove to have considerable far reaching value insofar as prevention of either of these two states is concerned, if we consider these factors alone may not only jeopardize overall health, longevity, and life quality, but foster a high risk for injuries such as hip fractures, expected to show an immense increase in prevalence among the elderly by 2050.
Aim
In light of the importance of helping older adults to maintain a high level of wellness and one free from excess fears and preventable health issues, this mini review sought to establish whether there is a role for improvements in frailty prevention and its possible link to excess fears of falling among older adult populations.
A parallel aim was not only to establish if more should be done in this regard, but if desirable, in what respect?
Hypothesis
It was hypothesized that a possible bidirectional relationship would be found to exist between frailty and fears of falling among a substantive proportion of older community dwelling adults. Moreover, a link for both frailty and falls fears to hip fracture risk would appear to be an apparent, albeit possibly preventable, important disabling pathway.
Relevance
Frailty, a potentially preventable serious health state and undisputed impediment to well-being among many older populations, not only impacts bone fragility, but overall energy levels, muscle strength capacity, and gait. Frailty also commonly engenders various degrees of anxiety, and depression 6 that alone or in combination with one or more of these factors can be expected to not only exacerbate frailty, but also associated levels of serious morbidity and excess rates of premature mortality, as well as possible parallel increases in falls risk, as well as fears of falling.
As such, the excess human as well as fiscal costs of frailty are currently immeasurable, and are likely to increase, rather than decrease, as societies age unless actions are taken to offset this possible cycle of highly adverse events. In particular, falls that often cause severe injury, anxiety and loss of confidence, as well as activity avoidance, depression, and social isolation due to ‘fears of falling’ a collective term denoting a set of negative beliefs that appears to occur in up to 85 percent of older adults who have experienced prior falls 7 undoubtedly tends to increase frailty or provoke its multiple manifestations 8. In particular, falls leading to hip fractures that occur frequently among the frail elderly not only predict less than desirable outcomes of survivors post hip fracture surgery 9, but the persistence of falls fears, anxiety, and low self-efficacy 10.
Rationale
Frailty, an age associated syndrome commonly attributed to under nutrition among other factors, appears strongly associated with a progressive decline in several physiological systems that can collectively heighten the older adult’s vulnerability to the risk of multiple adverse health events and outcomes, such as disability or death 11. In this regard, both frailty itself, as well as falls injuries often attributable in part to frailty features such as muscle and bone mass declines, and which often produce an excess of fears, such as falls related fears, can clearly be expected to lower the ability of the affected frail aging adult to adapt to one or more undesirable stresses as well as reducing the chances of successful aging and a high life of quality. Yet, for many older adults living in the community and who may slowly lose their independence, this remains an enormous personal problem, and is one clearly likely to markedly raise the immense and profound social costs associated its well established negative impact on function, as well as social and mental health status 12, 13, particularly if it contributes to a fragility hip fracture 11. In turn, as well as fostering an increased risk for falling or actual fall injuries leading to a fear of falling, fractures and further possible injuries and frailty or the onset of frailty, a deleterious perpetual cycle of adverse health outcomes can be expected to ensue. In this regard, although Malini et al. 13 found fear of falling in older adults to occur at high rates in this population, Malini et al. who found use of seven or more medications, having a hearing impairment, being functionally dependent in activities of daily living, diminished walking speed, fair and poor/very poor self-rated health and depressive symptoms to be key related health issues, did not discuss the factor of frailty directly in this respect. However, Crehan et al. 14 found a quarter of 47 elderly fallers who appeared to exhibit falls fears were also largely frail (75% cases), while in a study of older adults located in four Indian villages, among several associated factors mentioned as salient frailty determinants, such as low education, socioeconomic status and physical activity, age, being female, the frail elderly observed in that study tended to have a higher odds of falls as well as fear of falling compared to those designated as being non-frail, irrespective of the frailty definition 15. As well as falls, various fear perceptions, which have been studied for some time have shown the specific ‘fear of falling’ may in turn lead to the onset or perpetuation of a state of frailty, poor life quality, and a heightened falls risk and incidence of falls in their own right 16. Indeed, a fear of falling and/or low falls efficacy appears to be a key risk factor for frailty in older adults with and without diabetes 17, and is one suggesting this linkage may have a possible profound role to play in terms of clarifying those frailty determinants that might be modifiable, and their role should not be negated, but rather, should arguably be studied further in the future as indicated by Seematter-Bagnoud et al. 18.
Methods and Procedures
In accord with the aims of this report, the PUBMED, PUBMED CENTRAL, and GOOGLE SCHOLAR depositaries believed to house salient topical peer reviewed articles were carefully searched. Key terms used alone or in combination included, ‘aging’, ‘frailty’, ‘frail elderly’, ‘fear of falling’, ‘interventions’. No yearly restrictions were applied, and after an extensive scan of the available data, all pertinent reports addressing the current topic were scrutinized in detail, regardless of research design, and those deemed of substantive relevance were selected to provide an overview of this topic. The method of reporting in this instance was limited solely to a narrative descriptive format, given the low numbers of topical papers, or any substantive numbers of prospective studies on this topic. Excluded were foreign articles, proposals for future studies, nursing home studies, and issues related to frailty other than falls fears.
Search Results
The study of frailty has been pursued for more than four decades and as representative of the sub study topics covered, the inventory posted at PUBMED 1980-2021 and downloaded December 10, 2021 revealed a very modest number of articles linking frailty and falling fears as follows.
Among these, more than half were not relevant to the present discourse, or were study proposals. Those that were deemed relevant were categorized as being of general reports, versus research based reports.
General Observations
Among the articles relevant to the present topic, although limited in quantity, available data do appear to strongly support the view that many older adults are likely to be frail or in a pre frailty state, a recently constructed term and syndrome employed to characterize those vulnerable older adults who tend to exhibit an increased risk of premature or excess rates of functional declines, institutionalization, hospitalization, and death 1, 19. Other reports indicate that those older adults deemed to be frail, as well as those elderly who are deemed in robust health may yet both exhibit high rates of falling and possible subsequent fears of falling if they have incurred a an injurious fall or believe they are at risk for a future fall. Conceptually, this appears to set the stage for either magnifying the presence of or increasing its risk. In particular, those elderly who restrict their weight bearing activities and others out of falling fears and who may then inadvertently suffer excess muscle mass losses, bone mineral density alterations, weakness and lack of energy, depression, and a heightened medication need, among other negative frailty associated impacts may be highly vulnerable in this regard. Those who have studied this topic thus tend to agree that this series of overlapping events is undoubtedly of high importance to acknowledge in that once a cycle of falls and frailty is established, this situation can be expected to foster a high risk state for serious injuries, adverse health outcomes including falls 3, as well as possible subsequent increments in frailty 20, wherein there may be a further and more permanent loss of the well attuned harmonic interaction between multiple domains or dimensions of wellbeing including those of multiple genetic, biological, functional, cognitive, psychological and functional health domains 21.
In light of these highly negatively impactful events, including possible increases in hospitalizations, immense health care costs, and premature mortality rates 3, and the belief that neither frailty nor falls are inevitable, a fair number of current recommendations to offset this adverse cycle of events have been documented. These include the application of early screening as well as efforts to actively intervene to avert this negative cycle of interacting events as well as its various secondary health outcomes and cycle of excess suffering, including comorbidity and falls 21, 22.
What the Research Shows
Although frailty is often associated with functional declines, and is said to be distinguishable from aging and to confer a high risk for falls 22, 23, many studies of older adults currently reviewed, such as that by Tomita et al. 24, Makino et al. 25 and Lach et al. 26, did not discuss the attribute of frailty as a possible falls fear predictor in community dwelling elderly adults. In addition, the attribute termed ‘fears of falling’ also closely related to the risk as well as actual prevalence of falls among the elderly, was not mentioned in the context of a study focusing on frailty (eg., 27) As observed by Guedes et al. 22, Esbri-Victor et al. 28 who did assess the association between the attributes of fear of falling and frailty among 183 older Spanish adults with a prior falls history using validated questionnaires the authors found fears of falling to preside in over 76 percent of cases, with 55 percent indicating a high concern. Just over 88 percent of those deemed frail indicated they had a fear of falling with a relative risk of 3.18 compared to those who were not frail. Significant predictors after controlling for other variables were female gender and the presence of depression. Since this was a cross-sectional study, the cause-effect association between frailty and falls fears could not be established, however.
Nonetheless, work conducted in 1994 –did appear to open the door to the possibility that fear of falling, commonly generated in response to an actual fall, could possibly induce or heighten frailty, especially among those in the higher age ranges where falls related fears appear to rise incrementally 29. Again, this study, albeit a cross-sectional one, did tend to support the view that older community dwelling adults who feel depressed or dissatisfied with life, as well as those who experience falls, are likely to be more impacted as far as future falls risk and frailty are concerned 16. In addition, Ní Mhaoláin et al. 30 found frail fallers to suffer from an increased fear of falling when compared to the more robust faller (p < 0.001). Frail fallers also exhibited higher depression scores than non frail fallers, while fallers at a transitional level of frailty were deemed to represent a particularly vulnerable group psychologically speaking.
Delbaere et al. 31 who did conduct a prospective study of older adults from the perspective of falls fears, fears of movement and physical activity, and falling, was able to conclude that fear of falling had possible implications for the development of physical frailty, even though they did not actually assess frailty. They further affirmed those who were female and in the higher age groups were likely to be at most risk.
In their study, Silviera et al. 32, examining elderly fallers with varying frailty designations, found higher fear of falling perceptions in those deemed frail compared to those deemed non frail. As well, Kressig et al. 33 who noted symptoms of activity related fears of falling to be present among at least 50 percent of older adults deemed to be transitioning to frailty, also found these fears to be associated with depression, as well as prevailing levels of functional ability. Silviera et al. 32 further concluded that frailty is indeed often associated with a heightened fear of falling, as well as reduced muscle strength, and gait abnormalities deemed to possibly lead to falls, while Makino et al. 34 likewise conclude that frailty status may well predict future falls along with the fear of falling in older community-dwelling adults. Fear of falling that induces sedentary behavior is also likely to exacerbate the risk for incurring frailty states or worsening these, as well as falls, regardless of sociodemographic factors 35. Martin et al. 11 too conclude there are close associations between frailty, sarcopenia, osteoporosis and falls that warrant attention especially in cases where older adults have fallen or sustained a fracture or both, as these individuals may not only be frail and require a care plan involving both nutrition and exercises, but also require specific help to prevent future falls. Indeed, Higuchi et al. 4 found frail elderly who exhibited falling fears to be worse off physically speaking than those with no fear attributes. Other data reveal the fear of falling can not only contribute to psychological conditions such as depression, but can also impact on the health-related life quality of frail elderly people 36.
In short, therefore, although the literature on the current topic of interest is neither robust, nor conclusive, it appears hard to refute a case for the application of both timely as well as effective intervention strategies to prevent or reduce frailty among older vulnerable adults. This may not only help to reduce the chances of a high falls risk, but may also be beneficial for preventing excess frailty, future falls, as well as future falls fears among frail older adults 37 and should be studied in various contexts, and in diverse groups of older adults. Explicit attention to identifying and intervening upon excess falls fear beliefs where they prevail also seems imperative.
Indeed, a recent study of 175 China based community dwelling older adults from five districts 38 showed those study participants who reported having a fear of falling were 7.2 times more likely to be frail than those reporting no such fear, and among those sixty percent of cases deemed frail, eighty one percent affirmed they had a fear of falling. Similarly, Perez-Ross et al. 39 who examined 564 elderly people with a mean age of 76.05 years; and where 83.9 percent were deemed to be pre frail, among the four factors associated with frailty they included a fear of falling. Further findings of Alcolea–Ruiz et al. 40 tend to affirm that fear of falling is significantly elevated in the presence of frailty.
Hence, although frailty represents a highly challenging negative state of wellbeing among many older adults and one that clearly exposes the sufferer to a multitude of potentially preventable adverse health outcomes 41, it appears safe to say that excess frailty can. possibly be averted in part by multiple approaches that might include taking steps to minimize the onset or perpetuation of excess fears related to future falls among those elderly adults deemed most vulnerable. Conversely, in light of the rapidly ageing global population, and the parallel rise in frailty, as well as falls injuries and resultant possible fears of falling, the current social and economic burden of these two conditions alone will undoubtedly continue to rise exponentially if not addressed in a timely manner. In addition, due to associated increases in numbers of older adults living to higher ages, older adults with multi morbidities and those who survived COVID-19, soaring healthcare and social care costs and suffering can be anticipated if sporadic or belated preventive efforts remain the norm.
To address this issue, it is uplifting to see that while more needs to be done, sufficient research does point to the promise of improved health and social outcomes for the vulnerable elderly, through insightful and carefully tailored preventive approaches 42, 43, 44 that do currently exist. These include, but are not limited to multi-component community-based as well as home-based approaches and occupational therapy strategies designed to improve muscle and bone mass and function believed to help reduce both frailty as well as falls risk 39, 44, 45, 46, 47. As well as structured exercises, strength training, or physical activities that involve functional training and coordination exercises 48, structured nutrition interventions 49, and/or cognitive behavioral intervention approaches to reduce frailty, as well as falls and the fear of falling may similarly help to increase independence, confidence and energy 7, 37, 50. Further efforts directed towards reducing harmful medications, improving calcium and vitamin D status, diabetes control, and desirable home adaptations 44, 51, 52, efforts to provide a person-centered and goal setting approach 48 and encouraging social engagement 53 will also likely prove helpful, as will proactive careful screening to identify at risk adults 38, 53, 54. Programs that try to encourage personal development and growth, in spite of aging, and physical, social, emotional, and economic environments that foster wellbeing and active aging appear highly promising as well 55.
Discussion
While aging is inevitable, increasing evidence suggests aging as a negative state does not have to be a foregone ordained experience of downward spiraling events and perceptions. This review explored the possible contribution of fears of falling to frailty development and exacerbation, along with any observed frailty, falls risk associations with a view to providing more insight into opportunities to limit or avert some age associated adverse outcomes. These include, but are not limited to a heightened risk of disability, low levels of functional autonomy, high numbers and impact of one or more comorbid diseases, falls and falls injuries, plus multiple degrees of cognitive impairment.
On the other hand, while not definitive, and needing more careful study, it appears safe to say a fairly solid case can be made for the promise of dedicated efforts that attempt to prevent the risk of poor health status and outcomes attributable to frailty in elderly populations, including those elderly who exhibit persistent fears of falling and/or have fallen as a result of frailty. As well as preventing frailty where possible, preventing falls is strongly indicated as well, because even those older adults who are healthy, but incur a falls injury or an actual hip fracture injury, may be at risk for frailty that can perpetuate a downward spiral of health events, even though their association is clearly complex and largely likely to prove non linear and cumulative [see Figure 1].
Figure 1.Conceptual Model of Multiple Interrelated Factors Potentially Impacting Frailty Cumulatively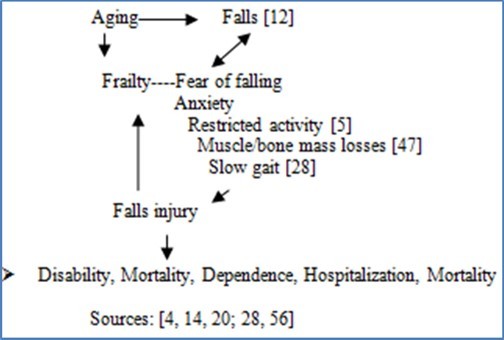
It is also evident that this is not only an urgent public and social health concern as a whole, but a promising new field of endeavor where most peer reviewed articles have been published within the last five years and among these several are successful studies that show frailty can be somewhat reversed 57. Moreover, those who are less frail are more likely to be more autonomous and less subject to falls injuries and sedentarity 55.
At the same time, and bearing in mind, insights, answers and optimal solutions take considerable time to emerge, attention directed towards those most vulnerable to frailty or becoming frail who appear to be women in the higher age groups, those living in poverty, those with low educational levels, living in unsafe housing who are underweight as well as those with diabetes, dementia, disability, and/or depression and that accepts disability is a part of aging 58, 59, as well as those that have a falls history 8, might be targeted preferentially using the most promising approaches examined in randomized studies. These include, but are not limited to various forms of physical activity; physical activity combined with nutrition; physical activity plus nutrition plus memory training; home modifications; pre-habilitation (physical therapy plus exercise plus home modifications) and comprehensive geriatric assessments 60.
Alternately, in light of the independent as well as collective impact of both frailty and falls fears on multiple personal dimensions of health, as well as the broader social and political dimensions of ‘wellbeing’ 55, the failure to address this burgeoning issue in an integrated rather than a fragmented manner will predictably produce higher levels of irreversible disability, hospitalization, low life quality, and premature deaths than not 36, 38. Moreover, since falls in their own right are not only increasing in numbers in the elderly, frailty which appears associated with falling and fear of falling to a high degree 56 can undoubtedly be expected to increase if associated fears of falling are neglected and inadvertently reduce activity involvement as well as involvement in rehabilitation interventions 52, 61.
To this end, ample evidence implies an urgent need for multiple far reaching collective efforts to better understand why some older adults are more vulnerable to frailty than others, and to more effectively discriminate and untangle the most promising potentially preventable antecedents using actionable preventative approaches. There must also surely be improved practical efforts to not only avert falls as well as falls fears, but to better understand the origins of falls attributable to excess fear that can prevail even in the absence of any actual overt falls experience. Based on the current literature, it also appears comprehensive assessments, longitudinal exploratory studies, plus an inter disciplinary approach, along with well designed efficacy studies that focus on heightening positive cognitions, provider knowledge, falls self-efficacy, efforts to counter the multiple negative mythologies of aging as purely a declining and negative economic state, plus personalized home-based one dimensional or multi component exercise interventions, and the provision of access to safe indoor and outdoor environments, efficacious social support, medication safety, and needed nutrient and educational resources will be especially helpful in this regard and are strongly encouraged 62, 63, 64, 65, 66, 67, 68.
Conclusions
Based on the Prevailing Data, it is Concluded that
I. Fear of falling is a potentially reversible correlate of frailty among the elderly.
II. Further research, plus personalized home-based community wide preventive efforts and treatments to address both frailty, as well as falls fears hold the potential to improve the lives of many older frail, as well as pre frail older adults as well as healthy adults.
III. Anticipated are enhancements in longevity, functional capacity, and life quality.
IV. Additional anticipated benefits are reductions in health care social and economic costs.
References
- 1.Xue Q L. (2011) The frailty syndrome: definition and natural history. Clinics in Geriatric Med 27(1), 1.
- 2.Solfrizzi V, Scafato E, Lozupone M, Seripa D, Schilardi A et al. (2019) Biopsychosocial frailty and the risk of incident dementia: The Italian longitudinal study on aging. Alzheimers Dement. Italian Longitudinal Study on Aging Working Group. 15(8), 1019-1028.
- 3.Hoogendijk E O, Afilalo J, Ensrud K E, Kowal P, Onder G et al. (2019) Frailty: implications for clinical practice and public health. , Lancet 394(10206), 1365-1375.
- 4.Higuchi Y, Sudo H, Tanaka N, Fuchioka S, Hayashi Y. (2004) Does fear of falling relate to low physical function in frail elderly persons?: associations of fear of falling, balance, and gait. , J Jpn Phys Ther Assoc 7(1), 41-7.
- 5.Dias R C, Freire M T, Santos E G, Vieira R A, Dias J M et al. (2011) Characteristics associated with activity restriction induced by fear of falling in community-dwelling elderly. Rev Bras Fisioter. 15(5), 406-413.
- 6.Soysal P, Veronese N, Thompson T, Kahl K G, Fernandes B S et al. (2017) Relationship between depression and frailty in older adults: A systematic review and meta-analysis. , Ageing Res Rev 36, 78-87.
- 7.Parry S W, Bamford C, Deary V, Finch T L, Gray J et al. (2016) Cognitive-behavioural therapy-based intervention to reduce fear of falling in older people: therapy development and randomised controlled trial - the Strategies for Increasing Independence, Confidence and Energy (STRIDE) study. Health Technol Assess. 20(56), 1-206.
- 8.McInnes E, Seers K, Tutton L. (2011) Older people's views in relation to risk of falling and need for intervention: a meta-ethnography. , J Adv Nurs 67(12), 2525-2536.
- 9.Inoue T, Maeda K, Nagano A, Shimizu A, Ueshima J et al. (2020) Undernutrition, sarcopenia, and frailty in fragility hip fracture: Advanced strategies for improving clinical outcomes. , Nutrients 12(12), 3743-10.
- 10.Visschedijk J, R van Balen, Hertogh C, Achterberg W. (2013) Fear of falling in patients with hip fractures: prevalence and related psychological factors. , J Am Med Dir Assoc 14(3), 218-220.
- 11.Martin F C, Ranhoff A H. (2020) Frailty and sarcopenia. Orthogeriatrics: The Management of Older Patients with Fragility Fractures [Internet] In: Falaschi P, Marsh D, editors , Cham (CH): 4.
- 12.Clegg A, Young J, Iliffe S, Rikkert M O, Rockwood K. (2013) Frailty in elderly people. , Lancet 381(9868), 752-762.
- 13.Malini F M, Lourenço R A, Lopes C S. (2016) Prevalence of fear of falling in older adults, and its associations with clinical, functional and psychosocial factors: The Frailty in Brazilian Older People‐Rio de Janeiro Study. , Geriatr Gerontol 16(3), 336-344.
- 14.Crehan F, O'Shea D, Ryan J M, Horgan F. (2013) A profile of elderly fallers referred for physiotherapy in the emergency department of a Dublin teaching hospital. , Ir Med 106(6), 173-176.
- 15.Kendhapedi K K, Devasenapathy N. (2019) Prevalence and factors associated with frailty among community-dwelling older people in rural Thanjavur district of South India: A cross-sectional study. , BMJ Open 9(10), 032904.
- 16.Arfken C L, Lach H W, Birge S J, Miller J P. (1994) The prevalence and correlates of fear of falling in elderly persons living in the community. , Am J Pub Hlth 84(4), 565-570.
- 17.B de Souza Moreira, Sampaio R F, Diz J B, A de Carvalho Bastone, Ferriolli E et al. (2017) Factors associated with fear of falling in community-dwelling older adults with and without diabetes mellitus: Findings from the Frailty in Brazilian Older People Study (FIBRA-BR). , Exptal Gerontol 89, 103-111.
- 18.Seematter-Bagnoud L, Santos-Eggimann B, Rochat S, Martin E, Karmaniola A et al. (2010) Vulnerability in high-functioning persons aged 65 to 70 years: the importance of the fear factor. Aging Clin Exp Res. 22(3), 212-218.
- 19.van Iersel MB, Jansen D R, Rikkert M G. (2009) Frailty in the elderly. Ned Tijdschr Geneeskd. 153, 183.
- 20.Merchant R A, Chen M Z, BLL Wong, Ng S E, Shirooka H et al. (2020) Relationship between fear of falling, fear-related activity restriction, frailty, and sarcopenia. , J Am Geriatr Soc 68(11), 2602-2608.
- 21.Pilotto A, Custodero C, Maggi S, Polidori M C, Veronese N et al. (2020) A multidimensional approach to frailty in older people. , Ageing Res Rev 60, 101047.
- 22.Guedes R C, Dias R, Neri A L, Ferriolli E, Lourenço R A et al. (2020) Frailty syndrome in Brazilian older people: A population based study. , Ciencia & Saude Coletiva 25(5), 1947-1954.
- 23.Lang P O, Michel J P, Zekry D. (2009) Frailty syndrome: A transitional state in a dynamic process. , Gerontol 55(5), 539-549.
- 24.Tomita Y, Arima K, Tsujimoto R, Kawashiri S Y, Nishimura T et al. (2018) Prevalence of fear of falling and associated factors among Japanese community-dwelling older adults. , Medicine (Baltimore) 97(4), 9721.
- 25.Makino K, Lee S, Bae S, Chiba I, Harada K et al. (2021) Simplified decision-tree algorithm to predict falls for community-dwelling older adults. , J Clin Med 10(21), 5184.
- 26.Lach H W. (2005) Incidence and risk factors for developing fear of falling in older adults. , Public Health Nursing 22(1), 45-52.
- 27.Won C W, Lee S, Kim J, Chon D, Kim S et al. (2020) Korean frailty and aging cohort study (KFACS): cohort profile. , BMJ Open 10(4), 035573.
- 28.Esbrí-Víctor M, Huedo-Rodenas I, López-Utiel M, Navarro-López J L, Martínez-Reig M et al. (2017) Frailty and fear of falling: The FISTAC study. , J Frailty Aging 6(3), 136-140.
- 29.Fundenberger H, Stephan Y, Hupin D, Barth N, Terracciano A et al. (2020) Prospective associations between subjective age and fear of falling in older adults. Aging Ment Health. 1-6.
- 30.Ní Mhaoláin AM, Fan C W, Romero-Ortuno R, Cogan L, Cunningham C et al. (2012) Depression: A modifiable factor in fearful older fallers transitioning to frailty?. , Int J Geriatr Psychiatry 27(7), 727-733.
- 31.Delbaere K, Crombez G, Vanderstraeten G, Willems T, Cambier D. (2004) Fear-related avoidance of activities, falls and physical frailty. A prospective community-based cohort study. , Age Ageing 33(4), 368-373.
- 32.Silveira T, Pegorari M S, de Castro SS, Ruas G, Novais-Shimano S G.Patrizzi LJ.(2015) Association of falls, fear of falling, handgrip strength and gait speed with frailty levels in the community elderly. Medicina (Ribeirão Preto). 48(6), 549-556.
- 33.Kressig R W, Wolf S L, Sattin R W, O'Grady M, Greenspan A et al. (2001) Associations of demographic, functional, and behavioral characteristics with activity‐related fear of falling among older adults transitioning to frailty. , J Am Geriatrics Soc 49(11), 1456-1462.
- 34.Makino K, Lee S, Bae S, Chiba I, Harada K et al. (2021) Prospective associations of physical frailty with future falls and fear of falling: a 48-month cohort study. Phys Ther. 101(6), 059.
- 35.da Silva VD, Tribess S, Meneguci J, Sasaki J E, Garcia-Meneguci C A et al. (2019) Association between frailty and the combination of physical activity level and sedentary behavior in older adults. , BMC Public Health 19(1), 709.
- 36.Suzuki M, Ohyama N, Yamada K, Kanamori M. (2002) The relationship between fear of falling, activities of daily living and quality of life among elderly individuals. , Nurs Hlth Sci 4(4), 155-161.
- 37.Chittrakul J, Siviroj P, Sungkarat S, Sapbamrer R. (2020) Multi-system physical exercise intervention for fall prevention and quality of life in pre-frail older adults: a randomized controlled trial. , Int J Environ Res Public Health 17(9), 3102.
- 38.Qin Y, Li J, McPhillips M, Lukkahatai N, Yu F et al. (2021) Association of fear of falling with frailty in community‐dwelling older adults: A cross‐sectional study. Nurs Hlth Sci.
- 39.Pérez-Ros P, Vila-Candel R, López-Hernández L, Martínez-Arnau F M. (2020) Nutritional status and risk factors for frailty in community-dwelling older people: A cross-sectional study. , nutrients 12(4), 1041.
- 40.Alcolea-Ruiz N, Alcolea-Ruiz S, Esteban-Paredes F, Beamud-Lagos M, Villar-Espejo M T et al. (2021) Prevalence of fear of falling and related factors in community-dwelling older people]. , Aten Primaria 53(2), 101962.
- 41.Cesari M, Calvani R, Marzetti E. (2017) Frailty in older persons. , Clin Geriatr Med 33(3), 293-303.
- 42.Tan P J, Khoo E M, Chinna K, Hill K D, Poi P J et al. (2014) An individually-tailored multifactorial intervention program for older fallers in a middle-income developing country: Malaysian Falls Assessment and Intervention Trial (MyFAIT). , BMC Geriatr 14, 78.
- 43.Gitlin L N, Winter L, Dennis M P, Hauck W W. (2008) Variation in response to a home intervention to support daily function by age, race, sex, and education. , J Gerontol A Biol Sci Med Sci 63(7), 745-750.
- 44.Pfortmueller C A, Lindner G, Exadaktylos A K. (2014) Reducing fall risk in the elderly: Risk factors and fall prevention, a systematic review. , Minerva Med 105(4), 275-281.
- 45.L De Coninck, Bekkering G E, Bouckaert L, Declercq A, Graff M J et al. (2017) Home‐and community‐based occupational therapy improves functioning in frail older people: A systematic review. , J Am Geriatrics Soc 65(8), 1863-1869.
- 46.El-Khoury F, Cassou B, Latouche A, Aegerter P, Charles M A et al. (2015) Effectiveness of two year balance training programme on prevention of fall induced injuries in at risk women aged 75-85 living in community: Ossébo randomised controlled trial. , BMJ.; 351, 3830.
- 47.Yoshimura N, Muraki S, Oka H, Iidaka T, Kodama R et al. (2018) Do sarcopenia and/or osteoporosis increase the risk of frailty? A 4-year observation of the second and third ROAD study surveys. , Osteoporos Int 29(10), 2181-2190.
- 48.Rasmussen R L, Holst M, Nielsen L, Villumsen M, Andreasen J. (2020) The perspectives of health professionals in Denmark on physical exercise and nutritional interventions for acutely admitted frail older people during and after hospitalisation. Health Soc Care Community. 28(6), 2140-2149.
- 49.Hsieh T J, Su S C, Chen C W, Kang Y W, Hu M H et al. (2019) Individualized home-based exercise and nutrition interventions improve frailty in older adults: A randomized controlled trial. , Int J Behav Nutr Phys Activity 16(1), 1-5.
- 50.Kapan A, Luger E, Haider S, Titze S, Schindler K et al. (2017) Fear of falling reduced by a lay led home-based program in frail community-dwelling older adults: A randomised controlled trial. , Arch Gerontol Geriatr 68, 25-32.
- 51.Carlsson G, Nilsson M H, Ekstam L, Chiatti C, Malmgren Fänge A. (2017) Falls and fear of falling among persons who receive housing adaptations-results from a quasi-experimental study in Sweden. Healthcare (Basel). 5(4), 66.
- 53.Walston J, Buta B, Xue Q L. (2018) Frailty screening and interventions: Considerations for clinical practice. , Clin Geriatr Med 34(1), 25-38.
- 54.Lee H, Lee E, Jang I Y. (2020) Frailty and comprehensive geriatric assessment. , J Korean Med Sci 35(3), 16.
- 55.Tornero-Quiñones I, Sáez-Padilla J, Espina Díaz A, Abad Robles MT, Sierra Robles Á. (2020) Functional ability, frailty and risk of falls in the elderly: Relations with autonomy in daily living. , Int J Environ Res Public Health 17(3), 1006.
- 56.Bahat Öztürk G, Kılıç C, Bozkurt M E, Karan M A. (2021) Prevalence and associates of fear of falling among community-dwelling older adults. , J Nutr Health Aging 25(4), 433-439.
- 57.Sadjapong U, Yodkeeree S, Sungkarat S, Siviroj P. (2020) Multicomponent exercise program reduces frailty and inflammatory biomarkers and improves physical performance in community-dwelling older adults: A randomized controlled trial. , Int J Environ Res Public Health 17(11), 3760.
- 58.St John PD, Montgomery P R. (2013) Acceptance of disability and the risk of frailty. , Can Geriatr J 16(3), 105-110.
- 59.Llibre Rodriguez JJ, Prina A M, Acosta D, Guerra M, Huang Y et al. (2018) The prevalence and correlates of frailty in urban and rural populations in Latin America, China, and India: A 10/66 population-based survey. , J Am Med Dir Assoc 19(4), 287-295.
- 60.MTE Puts, Toubasi S, Andrew M K, Ashe M C, Ploeg J et al. (2017) Interventions to prevent or reduce the level of frailty in community-dwelling older adults: a scoping review of the literature and international policies. Age Ageing. 46(3), 383-392.
- 61.Litwin H, Erlich B, Dunsky A. (2018) The complex association between fear of falling and mobility limitation in relation to late-life falls: A SHARE-Based Analysis. , J Aging Health 30(6), 987-1008.
- 62.Francisco M Martínez-Arnau, Prieto-Contreras Lucía, Pérez-Ros Pilar, Francisco M Martínez-Arnau, Lucía P C et al. (2021) Factors associated with fear of falling among frail older adults, Geriatric Nurs. 42(5), 1035-1041.
- 63.Apóstolo J, Cooke R, Bobrowicz-Campos E, Santana S, Marcucci M et al. (2018) Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: A systematic review. JBI Database System Rev Implement Rep 16(1), 140-232.
- 64.Calvo-Sotomayor I, Atutxa E, Aguado R. (2020) Who is afraid of population aging? myths, challenges and an open question from the civil economy perspective. , Int J Environ Res Public Health 17(15), 5277.
- 65.Pérez-Ros P, Vila-Candel R, Martínez-Arnau F M. (2020) A home-based exercise program focused on proprioception to reduce falls in frail and pre-frail community-dwelling older adults. , Geriatr Nurs 41(4), 436-444.
- 66.Duarte G P, JLF Santos, Lebrão M L, YAO Duarte. (2019) Relationship of falls among the elderly and frailty components. Rev Bras Epidemiol.21Suppl 02(Suppl 02):. 180017.
Cited by (4)
This article has been cited by 4 scholarly works according to:
Citing Articles:
Journal of Clinical Medicine (2025) OpenAlex
THE THERAPIST (Journal of Therapies & Rehabilitation Sciences) (2024) OpenAlex
THE THERAPIST (Journal of Therapies & Rehabilitation Sciences) (2024) Crossref