
The Prevalence of Intestinal Parasite Infection in El Behara Schoolchildren.
Abstract
This study was conducted to evaluate the prevalence of intestinal parasite in schoolchildren in Damanhur, Egypt and some of its villages. The pathogenic enteric protozoa have been progressively involved in bargaining the soundness of a great many individuals, for the most part in creating nations. Mediations are being set up to control the dreariness and mortality because of these protozoan contaminations. A portion of these mediations target school going kids with regards to class based wellbeing intercession. The present examination concentrated on exploring the commonness of intestinal protozoan contaminations among younger students chose networks comprising of urban, urban-poor and per urban settlements in the Damanhour and a few towns. In the present work Giardia lamblia was the second usually identified protozoan with a diseases rate 10.4% among the analyzed cases. In the present examination generally speaking level of parasitic contaminations among the kids was 57.3%. It's viewed as Enterobius vermicularis was the most usually identified protozoan as it spoke to 4.1% of the parasitic diseases in the considered cases pursued by Ascaris lumbricoides; 1.4% and Giardia lamblia contaminations as they spoke to 0.6%; separately. The protozoa like Giardia and Cryptosporidium are regularly present in surface waters and cause episodes in this manner legitimately affecting human wellbeing.
Article Information
- Received
- Accepted
- Published
Academic Editor: Patricio De los Ríos, Universidad Católica de Temuco, Chile.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Eman H. Radwan, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Eman H. Radwan, Faculty of Science, Damanhour University, Egypt —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Protozoa are eukaryotic cells distributed worldwide in nature and are receiving increasing attention as human and animal pathogens and potential vehicles for the transmission of bacteria in the environment. One of two persons in the world is affected by waterborne or foodborne parasites 1, 2, 3. Acanthamoeba is a genus of free-living amoebae (FLA), which are environmental eukaryotic cells distributed worldwide in nature 4, 5, increasing the risk of human illness caused by bacteria or Acanthamoeba. Acanthamoeba species are showing an increased role as human pathogens causing pneumonitis, and dermatitis 6, the infection routes are mostly from the environment. The Cryptosporidium species and Giardia intestinally are major pathogens in the waterborne transmission of infections and they are able to persist in the environment due to the robustness of the oocysts and cysts 7. Entamoeba histolytica is an anaerobic parasitic protozoan, part of the genus Entamoeba. Predominantly infecting humans and other primates, E. histolytica is estimated to infect about 50 million people worldwide. Intestinal protozoan infections are of public health importance globally, particularly among children of school going age and the immunocompromised 8, 9. Protozoan parasites contribute immensely to the burden of intestinal parasitic infections among children 10, 11. Poor hygiene coupled with children voracious eating habits particularly puts them at greater risk of acquiring these infections 12, 13. Transmission is by feco-oral route and most infections tend to be asymptomatic. The common symptoms include vomiting, abdominal discomfort and dysentery 14.The consequences of intestinal parasites among children particularly include malnutrition, poor physical and mental development, and cognitive and behavioral deficiencies 15, 16. It is believed that children of school going age forms the majority of them at risk population, and are therefore capable of maintaining the transmission of the infection in the community, particularly among their peers 17, 18.
Intestinal parasitic infections are major international health concerns, affecting approximately one fourth of the world population, they cause a large scale of morbidity and mortality in developing countries. In tropical and subtropical areas, three hundred millions are severally ill due to intestinal worms, and of these at least 50% are school age. Intestinal nematodes infect many of world's children and constitute a formidable public problem. Although helminthic infections are common, the infected children may suffer nutritional deficits, serious illness, cognitive impairment and occasionally death. More than one billion people worldwide are infected with one or more species of intestinal nematodes 19. Enterobius vermicularis was found in the appendices of children between the ages of 7 and 11 years 20, 21. Pinworms as many other gastrointestinal nematodes don't need to rely on a vector for transmission. Autoinfection usually occurs via ingestion of infectious eggs by direct anus-to-mouth transfer. This is facilitated by the perianal itch induced by the presence of pin worm eggs in the perianal folds and commonly occurs as a result of nail biting, poor hygiene, or inadequate hand washing. Ascariasis is the most common helminthic infection seen in human being as one fourth of the world population is infected 22. Although the clinical pictures of this illness mostly silent or with chronic symptomatology, the massive infection in children can give rise to serious complications that require surgical interference 23. More than 20,000 deaths occur in endemic areas per year, moderate infections cause stunting of linear growth and malnutrition in children. Ascaris lumbricoides is the largest of intestinal nematodes affecting human. It is most prevalent in the 5 to 9 years old group of preschool and young school children who are more frequently exposed to contaminated soil than adults. The incidence is approximately the same in both sexes 24. Ascaris infections can be detected by finding the characteristic Ascaris eggs in stool by direct saline preparation technique in heavy infections, while in light infections concentration techniques are required as formol ether concentration and MIFC techniques. Trichuris trichiura is the third most common nematodes of humans (Ascaris and Enterobius vermicularis are number one and two). Adult worms inhabit the large intestine of man mainly the caecum. Less commonly the appendix and colon, where they live embedding their anterior thin part inside the submucosa 25, 26. Trichuris trichiura cause irregular and nodular thickening of the wall of the colon, it damages enterocytes in the terminal ileum, appendix and caecum. It may cause obstruction of the lumen of the appendix. Secondary bacterial infection or protozoal infections e.g (Amoebiasis, Balantidiasis) may also occur 27. Light infections are asymptomatic as the worms live harmlessly in the caecum and appendix. But heavy infection especially in children between 2-6 years cause chronic diarrhea, epigastric pain, vomiting, distention, flatulence, anorexia, and loss of weight. Eosinophilia is usually moderate but eosinophils and charcot-leyden crystals are often abundant in the stools. In massive infection rectal prolapse may occur 28.
Filariform larvae enter the lymphatic system 29, they are carried by the blood to the lung, where the larvae burst out of the capillaries into the patient's main respiratory system. They migrate upwards where they are swallowed and carried down into the digestive tract to settle in the small intestine and mature into adults that deposit eggs 30. Infected patients complain from mild diarrhea and cramps, fever, leucocytosis, vomiting, general weakness, blood or mucus in stool. When the larvae migrate to the lungs and air passage, the patient may have symptoms ranging from a simple dry cough to fever, difficulty in breathing and coughing up blood or pus 31, 32. Inflamed appendix had been reported in two siblings (8 years and 7 years old) presented with chronic abdominal pain and similar physical findings. The surgical findings included inflamed appendix with a cross section of the parasite Strangyloides. Strongyloides appendicitis has occurred almost exclusively in areas endemic to the parasite 33. Strongyloides stercoralis infection is diagnosed by performing fecal examination to detect larvae by using; wet mount, Harada-Mori filter paper, Baermann method and the agar plate culture technique (APCT). The latter is the most reliable method for the detection of Strongyloides stercoralis.
Schistosoma haematobium was implicated as the causal agent of granulomatous inflammatory reaction with eosinophilia and fibrosis. Intramural oviposition was associated with frank acute appendicitis, and serosal involvement in peritoneal adhesions, with ileoileal intussusceptions in one patient 34. The actual role of schistosomal infection as a contributory factor in appendicitis is still open to debate but the diagnosis must be enterpreted in patients in the tropics with features of acute appendicitis or recurrent abdominal pain 35. Amebiasis is an infection of the large intestine caused by Entamoeba histolytica that infect 10% of the world's population resulting in 100.000 deaths per year 36. Although its prevalence is higher in poor developing countries having the lowest level of sanitation, the convenience of modern travel, high rates of emigration cause existence of high risk group in developed countries. Entamoeba histolytica affects all groups of people, regardless of age or sex. Amebiasis spreads through food and water that has been contaminated by human feces but it also spreads by person to person contact 37. The ameba exists in two different forms: the infective cyst or capsulated form and the trophozoite form. Trophozoite cannot survive once excreted in the feces, so it cannot infect others. In the digestive tract the cysts are broken open by digestive secretion releasing the mobile trophozoities. Once released within the intestine, the trophozoites multiply by feeding on intestinal bacteria or by invading the linning epithelium of the large intestine and the appendix 38. The trophozoites may remain inside the intestine, in the intestinal wall or it may be carried by blood to the liver, lung, brain or other organs 39. The ability of Entamoeba histolytica to produce pathological changes depends on several factors as the virulence of the infective strain of the parasite, the host resistance, the host nutritional status and the bacterial infection of the colon 40. Entamoeba histolytica is rare to occur. Giardia lamblia is the most common protozoal infection of humans worldwide 41 and the second most common parasite in the United States after pin worms 42, 43. The centers for disease control and prevention (CDC) estimated more than 2.5 million cases of giardiasis annually 44. Giardiasis is an infection of the small intestine of people and animals by a microscopic flagellated protozoan Giardia lamblia 45 that spread via contaminated water and food also by direct person to person contact. Giardiasis is more prevalent in children than adults because adults have a stronger immune system to fight the disease 46. Giardiasis causes diarrhea and weight loss, hypersensitivity reactions in the form of rashes and urticaria. The most chronic stages is associated with vitamin B12 malabsorbtion, disaccharidase deficiency and lactose intolerance 47, as a result of covering the intestinal epithelium by the trophozoites and degeneration or damage of the mucosal surface 48. Giardia lamblia may spread from the duodenum to the gall bladder and biliary ducts to cause cholecystits, cholangitis and granulomatous hepatitis. Human cryptosporidiosis is caused by infection with the Apicomplexa protozoan of the genus Cryptosporidia 49. Cryptosporidium is an intracellular protozoan, there are two main genotypes that induce infection in humans: C hominis and C parvum. It causes gastrointestinal disease in humans as well as animals such as cattle, cats and dogs. It is one of the most common parasitic infections in humans 50. Cryptospordium parvum is the main pathogen responsible for human infection, it infects both immunocompotent and immunocompromised individuals. Up to 30% of childhood infections are asymptomatic, thus children can be a reservoir and transmit infection to others. Infection occurs via feco-oral route, humans shed oocysts in their feces which are then ingested via contaminated food, water or inhaled. Autoinfection could occur. Diagnosis of Cryptosporidium depends on visualization of oocysts by stool examination after concentration using sheather-sugar solution. Oocysts are better visualized when stained by modified Ziehl Neelsen acid fast stain where the organism appears bright pink. Entero test and intestinal biopsy help in the diagnosis 51.
Aim of the present study; The first aim of this study was to detection of parasites from feces and water samples. The second aim was the survey for school students, age of (6-17) years in Beheira Governorate. Whereas the third aim was to study the soil samples and makes questionnaire for sources of drinking water and food. Detection any infective stage of the intestinal parasites contaminating the soil in school yard and other play ground in the study area.
Material and methods: The Study Site has been undertaken in Beheira Governorate as the first study in this area which can provide status of parasitic infections among students. Beheira Governorate located in the west of the Delta and is bordered to the north by the Mediterranean Sea and east by the Rasheed branch and to the west by the governorates of Alexandria. The Governorate of El-Beheira enjoys an important strategic location. It is located between the Rashid branch in the east and the governorates of Alexandria and Matrouh in the west and the Mediterranean Sea in the north and Giza governorate in the south. This study was conducted on several schools in Damanhour and some of its villages which were selected to be representative to most districts of the city. The schools included in the survey were namely; Bastarah Primary, Zawia Ghazal Preparatory, Primary and Zarkoun Primary and within Damanhour Random samples from the secondary military school, secondary namozagy boys and secondary namozagy girls. The staff members of the investigated schools were informed about the objective of the survey and the activities that would be undertaken, therefore headmasters, teachers and other staff was very helpful and formed an important role in collection of samples and required data.
Questionnaire
The questionnaire sheet was designed to cover a variety of items concerning personal, environmental data and socio-economic data of the examined students which can be related to parasitic infections. The socio-economic data (education and occupation of parents)52. A sample of 810 students (578 male and 232 female) whose ages ranged between 6 -17 years was selected by stratified random sample.
Collection of Samples
I. Stool and Urine Specimens
Each student was provided with two clean, dry and labeled plastic containers for urine and stool specimens, at the second day the specimens were collected and the relevant data were recorded in the designed questionnaire sheet. The students who didn't give specimens were excluded from the sample. The urine specimens were examined by centrifugation sedimentation technique in the laboratory of the villages and Dr. Zebada Desoqy laboratory on the same day of collection. Stool specimens were visually scanned for the presence of the parasitic worms, blood and mucus, about one gram of each stool specimen was placed in 10 ml plastic bottle and (Merthiolate - formaldehyde) solution was added until it almost filled the container except the neck.
II. Soil Samples
In order to conduct soil examination, 60 soil samples were collected (10 samples from the shaded area of each studied school yard, 20 samples from sporting club and 30 samples from the areas around the houses). About 100 g of each sample was divided into two parts, one for detection of larvae of parasites by using Baermann's technique on the day of collection and the other part was kept in the labeled plastic bag to be examined by sugar floatation technique to detect eggs of helminthes in the laboratory of Faculty of Science Damanhour University.
III. Water Sample
The minimal volume of water necessary for analysis of the presence of parasitic protozoa is 10 L, while there on upper limit. Published reports include volumes 600 L and even more, when analyzing drinking water 53, 54, 55. Sampling is carried out by collecting from a depth of (20-30) cm below the surface. It is recommended to avoid water layers close to the surface or sediment, as they can contain various biological materials such as plant matter and mud, which can block filters and /or interfere with downstream analysis. So 40 L water sample were collected (10 L of drinking water from Damanhour city, 10 L of drinking water from villages, 10 L from Damanhour canal and 10 L from Bastra village canal) for detection protozoa in water, in the same day of collection to examine.
Parastioligical Examination
I. Urine Examination
Centrifugal sedimentation technique 56, the urine specimen was snaked and transfered into centrifuge tube, and centrifuged at 1500 r.p.m. for two minutes. Decanted supernatant and the sediment was examined for the presence of ova, using the XI0 objective to screen the whole of the deposit.
II. Stool Examination
Collection and Macroscopic Stool Samples
Fecal samples were collected in clean plastic containers, mothers were asked to handle the sample immediately after being passed stool sampled were examined macroscopically for the color, odor, consistency and presence of mucous , blood or visible parasites.
Preservation
Fecal samples were immediately preserved by different methods: MF preservation: approximately 1gm of the stool was placed in a plastic bottle containing 5 ml merthiolate formalin solution 57, then the stool was thoroughly broken into the solution to ensure accurate preservation. 2- Formalin preservation: about 1 g of the stool was placed in a second bottle containing 3ml 10% formalin and mixed thoroughly 58, the bottles were firmly covered and labeled. 3 - Methanol fixation: a smear was made from each specimen, labeled and immediately fixed in methanol for 5 minutes.
Microscopic Examination
MF direct smear; The MF preserved sample was mixed and one drop was placed on slide, covered with coverslip and examined micaroscopically 57. Concentration technique: MF preserved samples were concentrated using merthiolate Iodine Formaldehyde concentration technique (MIFC) 59.
III. Soil Examination
IV. Water Examination
Filtration of collected water sample is necessary to concentrate the (oo) cysts into a volume suitable for further processing, usually measured in ml. For this purpose water can be filtered through nitrocellulose or polycarbonate membranes 54.
Data Analysis
Data were coded, tabulated and analyzed by researcher’s computer; the chi-squared test was used to test statistical significance of the produced results.
Results
The present study was carried out to study the prevalence of intestinal parasitic on several school children in Damanhour and some of its villages. The result of the present study has been illustrated under the following items; socio-demographic and environmental characteristics of the studied sample, prevalence of intestinal parasitic infection among cases, in stool samples, distribution of the studied cases according to gender, distribution of the studied cases according to demographic data and comparison between the two studied groups according to the overall distribution on intestinal protozoa infection by sex. (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6).
Figure 1. Ascaris egg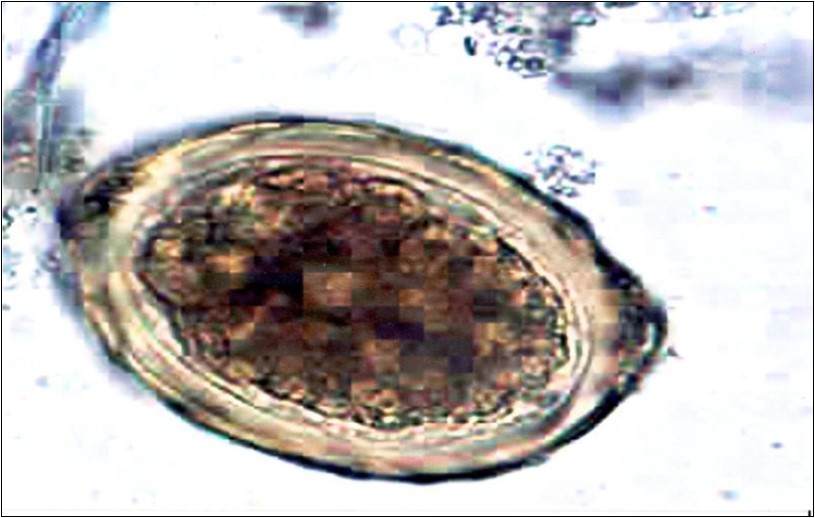
Download figure
Figure 2. Giardia cyst
Download figure
Figure 3. Hymanolepis nana egg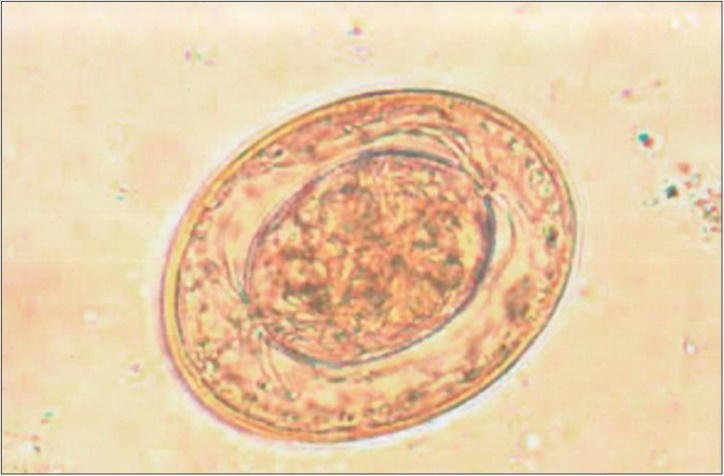
Download figure
Figure 4. Schistosoma mansoni egg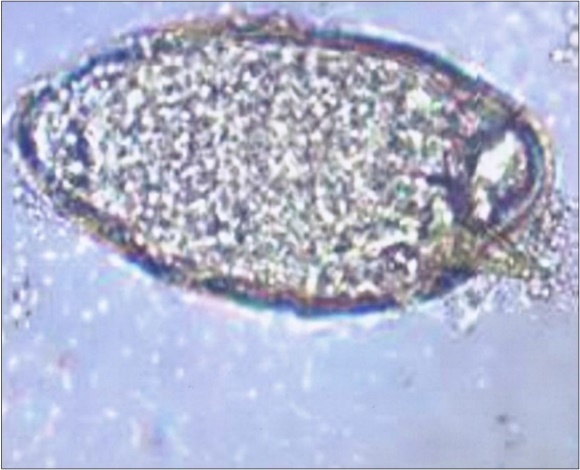
Download figure
Figure 5. Entamoeba histolytica Trovozoite
Download figure
Figure 6. Enterobius vermicularis egg
Download figure
The distribution of the studied cases according to gender in the present study included 810 children (578 male – 232 female) with sex ratio of 71.4:28.6 (Table 1). The comparison between the two studied groups according to infection was found that, the infected samples of 578 children were 61 samples by 10.6%, but for girls found that the infected samples of 232 are 30 samples by 12.9% (Table 2). The comparison between the two studied sex groups according to the overall distribution of intestinal protozoa infection showed types of parasites and their prevalence rates among examined students, two species of protozoa and five of helminthes were identified. Amongest protozoa Amoeba trophozoite the most frequent (1.3%) followed by Giardia lamblia (0.9%), Enterobius vermicularis was the most common helminth (4.1%) followed by Ascaris lumbricoides (1.4%) two cases of S. mansoni and only one case of H. nana was observed (Table 3). In the comparison between the four studied seasons according to infection was measured quarterly. The results showed that; in the summer, 275 samples were collected, of which 43 samples were infected with (15.6%), which is the highest percentage in the spring, 115 samples were collected, 10 of which were infected with an (8.7%). In the autumn, 254 samples were collected, of which 22 samples were infected with (8.7%). Finally, in winter, 166 samples were collected, 16 samples were infected with (9.6%) (Table 4).
Table 1. “The composition of the sample by gender”| no | % | |
| Total samples | 810 | 100 |
| Males | 578 | 71.4 |
| females | 232 | 28.6 |
| Infection | males | females | X2 | P | ||
| no | % | no | % | |||
| Non infected | 517 | 89.4 | 202 | 87.1 | 0.94 | 0.33 |
| Infected | 61 | 10.6 | 12.9 | 12.9 | ||
| Intestinalparasitic | Males(n=578) | Females(n=232) | Total(n=810) | X2 | P | |||
| no | % | no | % | no | % | |||
| E. vermicularis | 20 | 3.5 | 13 | 5.6 | 33 | 4.1 | 1.9 | 0.16 |
| E. coli | 0 | 0 | 0 | 0 | 0 | 0 | - | - |
| G. lamblia | 5 | 0.9 | 0 | 0 | 5 | 0.6 | 2 | 0.3 |
| H. nana | 1 | 0.2 | 0 | 0 | 1 | 0.1 | 0.4 | 1 |
| A. lumbricoides | 7 | 1.2 | 4 | 1.7 | 11 | 1.4 | 0.3 | 0.5 |
| E. histolitica | 0 | 0 | 0 | 0 | 0 | 0 | - | - |
| S. stercoralis | 0 | 0 | 0 | 0 | 0 | 0 | - | - |
| S. haematobium | 0 | 0 | 0 | 0 | 0 | 0 | - | - |
| Taenia spp. | 0 | 0 | 0 | 0 | 0 | 0 | - | - |
| T. trichiura | 0 | 0 | 0 | 0 | 0 | 0 | - | - |
| S. mansoni | 0 | 0 | 2 | 0.9 | 2 | 0.2 | 4.9 | 0.8 |
| H. heterophyes | 0 | 0 | 0 | 0 | 0 | 0 | - | - |
| Fasciola spp. | 0 | 0 | 0 | 0 | 0 | 0 | - | - |
| Amoeba trophozoite | 0 | 0 | 3 | 1.3 | 3 | 0.4 | 7.5* | 0.02* |
The distribution of the studied cases according to demographic data and show prevalence of parasitic infections among males and females in different age groups. In general, the males showed slightly higher rates of infection (60.1%) than female (39.9%). In the age ≤ 10 (6 – 10) Infection rate reaches (58.1%) and in age > 10 (11 -18) Infection rate reaches (41.9%) (Table 5). The distribution of the studied cases according to infect and parasite. This table shows that the percentage of infection E. vermicularis is higher than any other type where infection rate of (76.5%) followed by G. lamblia (11.8%) follwed by A.lumbricoides (8.8%) finaly, H.nana (2.9%)(Table 6). The relation between gender and age (n=148) showed that the percentage of parasites in the age of≤10 (6 – 10) in boys (61.8%) is higher than that of girls (52.5%), while the highest rate is >10 (11 – 18) years. The percentage of infection among girls (47.5%) is higher than that of boys (34%) (Table 7). The relation between gender with infect and parasite Infected male (27%) higher than female (16.9%) (Table 8). The relation between age with infect and parasite showed, in the age ≤10 (6-10) E. vermicularis (76.9%) and in the age of >10 (11-18) is (75 %) higher rates from any type of parasites (Table 9).
Table 5. distribution of the studied cases according to gender and age| no | % | |
| Gender | ||
| Males | 89 | 60.1 |
| Females | 59 | 39.9 |
| Age (years) | ||
| <10(6-10) | 86 | 58.1 |
| >10(11-18) | 62 | 41.9 |
| Min – Max | 6.0-18.0 | |
| Mean ±SD | 11.2±3.4 | |
| no | % | |
| Infection | ||
| Non infected | 114 | 77 |
| Infected | 34 | 23 |
| Parasites | ||
| E. vermicularis | 26 | 76.5 |
| G. lamlia | 4 | 11.8 |
| A. lumbricoides | 3 | 8.8 |
| H. nana | 1 | 2.9 |
| Age (years) | gender | Test of significance | P | |||
| Males (n=89) | Females (n=59) | |||||
| no | % | no | % | |||
| <10 (6-10) | ||||||
| >10 (10-18) | 55 | 61.8 | 31 | 52.5 | X2=1.2 | 0.26 |
| Min –Max | ||||||
| Mean ± S.D. | 34 | 38.2 | 28 | 47.5 | T=0.74 | 0.46 |
| Gender | X2 | P | ||||
| Males (n= 89) | Females (n= 59) | |||||
| no | % | no | % | |||
| Infection | 2.0 | 0.15 | ||||
| Non infected | 65 | 73 | 49 | 83.1 | ||
| Infected | 24 | 27 | 10 | 16.9 | ||
| Parasites | ||||||
| E. vermicularis | 17 | 70.8 | 9 | 90 | ||
| G. lamblia | 4 | 16.7 | 0 | 0 | ||
| A. lumbricoides | 2 | 8.3 | 1 | 10 | ||
| H. nana | 1 | 4.2 | 0 | 0 | 2.3 | 0.6 |
The Relation between age with infect and parasite E. vermicularis and G. lamblia Min(6%)-Max (17%) followed by A. Lambricoides Min (7%)-Max (14%) (Table 10). The prevalence of intestinal parasitic infections in relation to socio-economic classes of the examined students. It was found a statistically significant relation between parasitic infection and socio-economic classes of examined students, whereas the highest rate of infection (48.7%) was among the students of low socio-economic class compared to those of middle (26.1%) and high class (20.9%), (Table 11). The prevalence of intestinal parasitic infections among examined students in relation to the educational level of their fathers. The results indicated inverse correlation between parasitic infection and educational level of father, where the students belonged to illiterate or read and write fathers showed the highest rate of infection (50.6%) as compared to the students whose fathers were primary or preparatory educated (20.2%) and the students whose fathers were secondary or university educated (21.5%) this difference was statistically significant (Table 12). The prevalence of intestinal parasitic infections among examined students in relation to the educational level of their mothers. The results indicated inverse correlation between parasitic infection and educational level of the mothers, where the students belonged to illiterate or read and write mothers showed the highest rate of infection (48.2%) as compared to the students whose mothers were primary or preparatory educated (33.9%) and the students whose mothers were secondary or university educated (19.6%) this difference was statistically significant, (Table 13).
Table 10. The distribution of the different parasitic infections by age| Socioeconomic classes | infection | free | total | |||
| no | % | no | % | no | % | |
| Low | 169 | 48.7 | 178 | 51.2 | 347 | 100 |
| Middle | 76 | 26.1 | 215 | 73.8 | 291 | 100 |
| High | 36 | 20.9 | 136 | 94.7 | 172 | 100 |
| Total | 281 | 35 | 529 | 65 | 810 | 100 |
| Educational levels of their fathers | Examined students | total | ||||
| Infected | free | |||||
| no | % | no | % | no | % | |
| Read and write | 165 | 50.6 | 161 | 49.3 | 326 | 100 |
| Primary or preparatory education | 18 | 20.2 | 71 | 79.7 | 89 | 100 |
| High school or University education | 85 | 21.5 | 310 | 78.4 | 395 | 100 |
| total | 268 | 33 | 542 | 67 | 810 | 100 |
| Educational level of their mothers | Examined students | total | ||||
| Infected | free | |||||
| no | % | no | % | no | % | |
| Read and write | 170 | 48.2 | 182 | 51.7 | 352 | 100 |
| Primary or preparatory Education | 19 | 33.4 | 37 | 66 | 56 | 100 |
| High school or University education | 79 | 19.6 | 323 | 80.3 | 402 | 100 |
| Total | 268 | 33 | 542 | 67 | 810 | 100 |
Results of urine samples: The total number of examined urine samples 50 samples from students. Examination of this samples showed that all samples were free from eggs of the parasites. The total number of examined soil samples were; (10) samples from each studied school yard, (20) samples from sporting club, and (30) samples from the area around the house. Examination of these samples showed that all samples were free from eggs of the parasites. Result of drinking water sample: It is natural to have protozoa in the water of the canals both in the city and in the villages, but the strangest ones are found in drinking water Giardia lamblia was found in the drinking water samples.
Discussion
Parasitic sicknesses keep on being a noteworthy general medical issue particularly in youngsters 62. Being a reason for ailing health, development hindrance, pallor and perhaps different lacks could result in diminished efficiency and poor academic accomplishment 63. Parasitic sicknesses might be a reason for other medical issues, for example, a ruptured appendix, cholicystitis, and intestinal obstacle. The present examination was intended to explore the commonness of parasitic diseases among worked understudies by stool investigation. In the present examination in general level of parasitic contaminations among the youngsters was 57.3%. In Turkey the outcomes were in concurrence with the present examination which was 53% 64. In Riyadh, Saudi Arabia, the rates of parasitic contaminations were 42.2% in urban territories and 47.1% in zones where sewage is arranged in open channels 65. In Egypt, parasitic contamination among school age kids extended from 7.3%-30% 66, 67. Yassin et al. 68 from Gaza detailed that this rate was 27.6% when stool example was handled by direct smear and zinc sulfate floatation strategy and formol ether sedimentation method. Comparative rates were accounted for in Brazil in 2000 69, and in Quetta Pakistan (27.6% and 31%; individually 70.
The distinction in these rates of parasitic diseases in various nations might be influenced by various natural and epidemiological elements. Potentiating hazard factors incorporate feco-oral, air borne transmission and soil transmission in school age people. The high level of parasitic diseases in the present examination might be ascribed to terrible individual cleanliness of the contemplated test "school age kids". Low financial standard additionally influences their wholesome status and thusly lessens protection from contamination with crafty pathogens. Beside high rates watched might be because of the mix of various procedures done in the present investigation which encourage the determination of various kinds of protozoa. As to variety of intestinal parasitic contamination among kids, the present work uncovered that 49% of inspected cases harbored one parasite. In concurrence with the present investigation, it was discovered that 69.1% of tainted understudies in the Red Sea Governorate, Egypt were contaminated with one parasite, 22.5% and 7.6% were contaminated with two and three parasites individually 71.
In the present work, various procedures "formal ether focus, trichrome stain agar plate culture and Hematoxylin and Eosin recolor strategies" were utilized for examination of feces tests and ppendiceal content. It was discovered that Enterobius vermicularis and Ascaris lumbricoides diseases speak to 4.1% and 1.4% separately. This is demonstrative of the spread of wellbeing mindfulness in the home and school, where there is little proof of damage contrasted with earlier years. The high pervasiveness of Enterobius vermicularis might be because of the genuine increment in water borne contamination water borne malady. The little size of Enterobius vermicularis egg makes them hard to be dispensed with from polluted water even by utilizing filtration framework 72. Chlorine sanitization, which has incredibly added to the decline in water conceived ailment coming about because of pathogenic microorganisms in the water supply has no impact on Enterobius vermicularis and Giardia lamblia blister. Such oocyst has an invulnerable divider that opposes different burdens and chlorine cleansing 73. Fayad et al. 74 expressed that Cryptosporidium was perceived as a typical enteric pathogen among diarrhoeic youngsters in Egypt. In Zagazig Governorate, Egypt, a predominance of 16.7% was accounted for among youngsters matured from 2-12 years 75. Since the investigation test having a place with school age kids and their wholesome status is relied upon to be low and the parasitic diseases among them may impact the respectability of invulnerable framework rendering them increasingly vulunerable to secure cryptosporidiosis 76. Thus, absence of explicit treatment and general wellbeing consciousness of cryptosporidiosis in contrast with other intestinal protozoa as G. lamblia and E. histolytica may represent high contamination rate of Cryptosporidium 77.
In the present investigation, protozoal diseases were more typical than helminthes, this might be credited to the distinction in their method of transmission, the vast majority of sore or growths of protozoa are transmitted legitimately starting with one individual then onto the next. The transmission of most helminthes requires a middle of the road have, an outside hatching for development of infective stages 78. It's viewed as Enterobius vermicularis was the most ordinarily recognized protozoan as it spoke to 4.1% of the parasitic contaminations in the contemplated cases pursued by Ascaris lumbricoides; 1.4% and Giardia lamblia diseases as they spoke to 0.6%; separately. Mc Carthy et al. 79, feature the potential general wellbeing hugeness of endemic obtrusive amoebiasis in view of its high transmissibility in setting where cleanliness is imperfect. The present investigation has faith in particular screening and fitting treatment of patients and contacts. It was found India revealed that the commonness of Entamoeba histolytica in appendectomized kids was (1.4%) 80. In Czechoslovakia, Cerva et al,81 expressed that Entamoeba coli speak to 1 % of appendectomized cases. The present work Giardia lamblia was the second regularly identified protozoan with a diseases rate 10.4% among the inspected cases. Giardia was analyzed in 9% of grade younger students in Alexandria 82, and in Saudi Arabia. In Guinae, 8.6% of urban outpatients had giardiasis 83. Further low rate coming to down to 2.2% was accounted for in Gaza 84. The high rates of giardiasis can be disclosed by its protection from the chlorine level in typical faucet water 85. The commonest helminthic contamination identified in our investigation, was Enterobius verrnicularis. It was accounted for that 30% of the youngsters worldwide are contaminated with Enterobius verrnicularis86.
Wiebe 87 demonstrated that pinworms can enter effectively through the flawless inside divider, along these lines, it is relied upon to attack informative supplement. It was accounted for that its quality in reference section can give side effects of intense an infected appendix 88. Al Rabiah et al. 89 from Saudi Arabia revealed 3% histo-pathologically demonstrated instances of Enterobius verrnicularis among 201 appendectomy example. In England, it was accounted for to be 2.7% 90. Arca et al.91 from USA announced that the relationship of Enterobius verrnicularis contamination with intense an infected appendix shifts from 0.2-41.8% around the world. An examination done in Turkey demonstrated that Enterobius verrnicularis present in 3.8% of appendectomized kids 92. In the present work Ascaris lumbricoides was available in 1.4% of inspected cases. An examination done among younger students in Alexandria, it was discovered that the disease rates of Trichuris trichiura and Ascaris lumbricoides were 9.1% and 2.5%; separately 93. In Venzuela, it was accounted for that Ascaris lumbricoides present in 7.4% of appendectomized cases, and Trichuris trichiura present in 5.4% of them 94. In the present work H. nana was available in 0.1% of inspected cases. While as in Ismailia H. nana were accounted for among 5.5% of younger students 95, Dakahlia 5% 96 and Alexandria 2.2% 97.
As respect the sociodemographic parameter and parasitic contamination among the considered example no factually huge distinction was recognized between both genders. The present examination uncovered that the most elevated level of parasitic contaminations was among patients under 10 years, this could be ascribed to their terrible clean practices. It was trailed by 10-14 years classification, this can be clarified by their eating out entryway propensities. In Assiut, Abdel-Hafez 98 revealed that infective parasitic maladies were serious issue especially among the more youthful age gathering and those of low financial status. In Gaza, Shubair et al.99 demonstrated that kids matured 6-7 years were the most powerless age bunch obtaining parasitic contaminations. An examination done in Iran in 2003, demonstrated that the most helpless age to parasitic diseases was under 10 years of age, at that point the rate of contamination diminished bit by bit and the least contamination rate was among 14-15 years of age 100. As respects the instructive dimension of the mother, the present examination uncovered that the level of parasitic diseases was higher among kids whose moms were of lower and medium classifications of training than the individuals who have advanced education, this can be clarified via inconsiderateness of moms, This is demonstrative of the spread of wellbeing attention to the informed moms of their youngsters. Despite what might be expected, in Alexandria, higher rates of diseases were found among youngsters whose guardians were uneducated or simply perused and compose (41.3% and 56%; separately) 101. In Mexico, kids having a place with lower pay families and with less instructed moms had higher rates of intestinal parasitism 62.
References
- 1.Moss J A, Snyder R A. (2011) Pathogenic Protozoa," in Microbial Source Tracking: Methods, Applications,and Case Studies. , C Hagedorn,AR Blanch,VJ Harwood, Eds, Springer,New York,NY,USA 157-188.
- 2.Baldursson S, Karanis P. (2011) Waterborne transmission of protozoan parasites: review of worldwide outbreaks—an update 2004-2010,". , Water Research 45(20), 6603-6614.
- 3.Onichandran S, Kumar T, Lim YAL. (2013) Waterborne parasites and physico-chemical assessment of selected lakes in Malaysia,". , Parasitology Research 112(12), 4185-4191.
- 4.Adamska M. (2015) Molecular characterization ofCryptosporidiumandGiardiaoccurring in natural water bodies in Poland,". , Parasitology Research 114(2), 687-692.
- 5.Balderrama-Carmona A P, Gortares-Moroyoqui P, L H Alvarez-Valencia. (2014) Quantitative microbial risk assessment ofCryptosporidiumandGiardiain well water from a native community of Mexico,". , International Journal of Environmental Health Research 1-13.
- 6.Abd H, Shanan S, Saeed A, Sandstrom G. (2012) Survival of Vibrio cholerae inside Acanthamoeba and detection of both microorganisms from natural water samples may point out the amoeba as a protozoal host for V. cholerae,". , J of Bacteriology & Parasitology vol, 1-003.
- 7.Shanan S, Abd H, Hedenstrom I, Saeed A, Sandstrom G. (2011) Detection of Vibrio cholerae and Acanthamoeba species from same natural water samples collected from different cholera endemic areas in Sudan,". , BMC Research Notes 4, 109.
- 8.Gelaw A, Ana gaw B, Nigussie B, Silesh B, Yirga A et al. (2013) Prevalence of intestinal parasitic infections and risk factors among schoolchildren at the University of Gondar Community School, Northwest Ethiopia: a cross-sectional study. , BMC Public Health 13(304), 1-7.
- 9.R Simiyu CI Odhiambo DO Nanyu V Chege P Downing. (2013) Webuye Health and Demographic Surveillance Systems Baseline Survey of Soil-Transmitted Helminths and Intestinal Protozoa among Children up to Five Years. , Journal of Tropical Medicine. 2013.Article ID 734562, 1-7.
- 10.Harhay M O, Horton J, Olliaro P L. (2010) Epidemiology and control of human gastrointestinal parasites in children. Expert Rev Anti Infect Titer. 8(2), 219-234.
- 11.Hotez P J, Kamath A. (2009) Neglected tropical diseases in sub-saharan Africa: review of their prevalence, distribution, and disease burden. , PLoS Negl. Trap. Dis 3(8), 412.
- 12.Carvalho-Costa F A, Goncalves A Q, Lassance S L.(2007).Giardia lambliaand other intestinal parasitic infections and their relationships with nutritional status in children in Brazilian Amazon. Rev Inst Med Prop Sao Paulo. 49(3), 147-53.
- 13.UN1CEFWHO. (2009) Diarrhoea: Why children are still dying and what can be done. Geneva 27, Switzerland. www.unicef.org/media/files/Final_Diarrhoea_Report_Octob er_2009_final.pdf.
- 14.Schunk M, Jelinek T, Wetzek K, Nothdurff H D. (2001) Detection ofGiardia lambliaandEntamoeba histolyticain Stool Samples by Two Enzyme Immunoassay. , Eur. J. Clin. Microbial. Infect. Dis 20, 389-391.
- 15.Balci Y I, Turk M, N Polat Y Erbil. (2009) The distribution of intestinal parasites among children in Denizli. , Turkish J Pathol 33(4), 298-300.
- 16.Pedersen F K, Moller N E. (2000) Diseases among refugee and immigrant children. Ugesk Laeger. 162, 6207-6209.
- 17. (2006) WHO Preventive chemotherapy in human helminthiasis. Coordinated use of antihelminthic drugs in control interventions. A manual for professionals and programme managers. , Geneva: World Health Organization; 63.
- 18.Matthys B, Bobieva M, Karimova G, Mengliboeva Z, Jean-Richard V et al. (2011) Prevalence and risk factors of helminths and intestinal protozoa infections among children from primary schools in western Tajikistan. , Parasites & Vectors 4(195), 1-13.
- 19.Drake L J, Bundy D A. (2001) Multiple helminth infections in children: Impact and control. , Parasitology; 122, 973-81.
- 20.Lee K J, Lee I Y.Im K (2000).Enterobius vermicularisegg positive rate in a primary school in Korea. , Korean J Parasitol 38, 177-8.
- 23.Gil J M, Esturo G M, Ayala R P. (2006) Intestinal obstruction Due toAscariasis. , Int J of Surg; 8(2), 12-3.
- 24.Wiley Johan, Sons. (2010) Abdominal complications ofAscaris lumbnicoidesinfestation in children. Available from http://www3.interscience.wiley.com/journal , J.H. Louw 53, 518-31.
- 25.Garcia L S. (2001) . Diagnostic Medical parasitology, 4th Ed., ASM press , Washington, D.C 17-20.
- 26.Stephenson L S, Holland C V, Cooper E S. (2000) The public health significance ofTrichuris trichiuraCambridge journals. 121, 573-95.
- 27.Lintula H, Kokki H, Vanamo K. (2001) Single-blind randomized clinical trial of laparoscopic versus open appendectomy in children. , Br J Surg; 88, 510-4.
- 28.Hong S T, Lim H S, Kim D H, Kim S J. (2003) A case of gastroentenitis associated with gastric trichiuriasis. , J. KO 18, 429-32.
- 29.Masseau A, Hervier B, Leclari F. (2005) {Stongyloides sterconalis infection simulating polyarthritis nodosa). Rev Med Interne. 26(8), 661-3.
- 30.Lam C S, Mk Tong, Km Chan, Siu Y P. (2006) Disseminated strongyloidiasis: a retrospective study of clinical cause and outcome. , Eur J Clin Microbiol infect Dis 25(1), 14-8.
- 31.Lim S, Katz K, Krajdan S. (2004) Complicated and fatal strogyloides infected Canadians: risk factors, diagnosis and management. , CMA J 5, 479-84.
- 32.New berry AM, Williams D N, Stuffier W N. (2005) Strongyloides hyperinfection presenting as acute respiratory failure and gram-negative. Sepsis chest;. 128(5), 368.
- 33.Adedayo O, Grell G, Bellot P. (2002) Hyperinfective strongyloidiasis in the medical ward: review of 27 cases in 5years. , South Med J; 95(7), 711-6.
- 35.Doudier B, Parola P, Dales P, Linzberger N. (2004) Schistosomiasis as an unusual cause of appendicitis. , Clin Microbiol Infect; 10, 89-91.
- 36.Payman M D. (2007) Amebiasis presenting as acute appendicitis. Available from © , Lippincott Willia Wilkins. http://www.medscape.com/viewarticle/56690/3, South Med J; 100(11), 1140-2.
- 37.Rebecca J. (2006) Amebiasis: causes and symptoms. Medical Encyclopedia; 8: 14. Available from http://www. answers. com/ topic/ amebiasis-cuases and symptoms?cat=health.
- 39.Haque R, Mondal D, Duggal P. (2006) Entamoeba histolyticainfection in children and protection from subsequent amebiasis;. 74(2), 904-9.
- 40.Misra S P, Misa V, Dwivedi M. (2004) Factors influencing colonic involvement in patients with liver abscess. Gastro intestinal Endosc 59(4), 512-6.
- 41.Giardiasis. (1992) Surveillance. United States. Available from: www.cdc. gov/ mmwR/ priview/ mmwrhtml/ss4907a/.htm , CDC
- 42.DV Katz DE and Taylor. (2001) Parasitic infection of the gastrointestinal tract. , Gastroenterol Clin North Am; 30, 795-815.
- 43.Leder K, Weller P. (2002) Giardiasis. In: Rose BD, ed Infectious disease. , Wellesley, Mass:uptodate
- 44.Centers for (1992) Disease Control and prevention. Publication of CDC surveillance summaries. , MMWR Morb Mortal Wkly Rep 41(8), 145-6.
- 45.Glaser C, Lewis P, Wong S. (2000) Pet., Animal and vector-borne infections. , Pediatr Rev 21, 219-32.
- 47.Steiger U, Weber M. (2002) Ungewohuliche ursache vonerythema nodosum, pleuraerguss and reaktiver arthritis: Giardia lamblia (unusual etiology of erythema nodosum, pleural effusion and reactive arthritis:. Giardia lamblia) Schweiz Run dsch Med Prax; 91, 1091-2.
- 48.Abdull Ghaffar Murray. (2000) Intestinal and luminal protozoa pathogenesis. (3rd ed.) 2000; (3): 619-31.Available from: http://www.cdc.gov/Nicdod/dpd/parasites/giardiasis/factshtgiardia.htm.
- 49.Bushen O Y, Lima A A, Guerrant R L. (2006) Tropical infectious diseases. Principle pathogens, and practice Philadelphia, PA.; Elsevier-Cnurchill living st one;. , Cryptosporidiosis. In: Guerran 1003-14.
- 50.Blackburn B G, Mazurek J M, Hlavsa M. (2006) associated with ozonated apple cider. Emerg Infect Dis. 4, 684-6.
- 51.Ramirez N E, World L A, Sreevatsan S. (2004) A review of the biology and epidemiology of cryptosporidiosis in humans and animals. , Microbiol Infect 6(8), 773-85.
- 52.Fahmy S L, El-Sherbiny A F. (1983) Determining Simple Parameters for social classifications for health research. , Bull HIPH; 13, 95-107.
- 53.Medema G J, schijven J F. (2001) Modelling The swage discharge and dispersion ofCryptosporidiumandGiardiain surface water. , Water Res 35(18), 4307-4316.
- 54.Ali M A, Al-Herrawy A Z, El-Hawaary S E. (2004) Detection of eteric viruses,GiardiaandCryptosporidiumin two different types of drinking water treatment facilities. , Water Res 38(18), 3931-3939.
- 55.Karanis P, Sotiriadou I, Kartashev V, Kourenti C, Tsvetkove N et al. (2006) Occurrence ofGiardiaandCrptosporidiumin water supplies of Russia and Bulgaraia Environ. , Res 102(3), 260-271.
- 57.Sepero J J, Lawless D K. (1953) The "MIF" stain-preservation technique for the identification of intestinal protozoa. , Am J Trop Med Hyg; 2, 613-619.
- 59.Garcia L S, Bruckner D A. (1988) Macroscopic and microscopic examination of faecal specimens. In: Diagnostic Medical Parasitology.New. , York: 384-387.
- 60.Lima J P, Delgado F G. (1961) Diagnosis of strongyloidiasis, importance of Baermann’s method . , Am J Dig Dis; 6, 899-904.
- 61.Groenen G. (1992) epidemiology ofAscarisand its relevance to environmental health programmes. Quoted from Schulz S, Kroeger A. soil contamination withAscaris lumbricoideseggs as an indicator of environmental hygiene in urban areas of north-east Brazil. , J Trop Med; 95-103.
- 62.Quihial L, Valencia M E, Crompton D W, Phillips S, Hagan P et al. (2006) Role of the employment status and education of mothers in the prevalence of intestinal parasitic infections. , Mexico, BMC Public Health; 6, 225.
- 63.Simeon D, Callender J, Weng M, Granthan-McGregor S, Randath D D. (1994) School performance, nutritional status and trichuriasis in Jamaica school children. , Acta Pediatr; 83, 1183-93.
- 64.Mustafa M L, Adnan S Ukanliglil. (2003) Demographic and parasitic infection of school children and sanitary condition in San luirfa. , Turkey. J List, BMC Public Health 3, 6.
- 65.Al-Shammari S, Khoja T, El-Khwasky F, Gad A. (2001) Intestinal parasitic diseases in Riyadh, Saudi Arabia: Prevalence associates. , Trop Med Int Hlth 6(3), 184-9.
- 66.Abdel-Rahman E S. (2000) Intestinal parasites in different groups of immunocompromised children. Master of Pediatrics Thesis, faculty of Medicine Alexandria.
- 67.Hegab M H, Zamzam S M, Khater N M, Tawfeek D M, Abdel-Rahman H M. (2003) Opportunistic intestinal parasities among children with chronic liver disease. , J Egypt Soc parasitol; 33(3), 969-77.
- 68.Yassin M H, Shubair M E, AL-Hindi A I, Jadallah S Y. (1999) Prevalence of intestinal parasites among school children in Gaza City, Gaza Strip. J Egypt Soc Parasitol. 29(2), 365-73.
- 69.FM Martins de Paula, Elisio de Castro, pries MF Goncalves, Marcal M G, DMB Gampos et al. (2000) Parasitological and immunological diagnosis of strongyloidiasis in immunocompromised and non immunocompromised children at Uberlandia, state of Minas Gerais, Brazil Rev Inst Med Trop S Paulo;. 42(1), 51-5.
- 70.Al Wadood A, Bari Abdul.Abd El Rhman, Khawafa FQ (2005). Frequency of intestinal parasitic infection in children hospital. , Quetta, Pakistan, J Med Res.; 44(2), 30-5.
- 71.WML Kishk. (1998) Study of parasitic infections among Ras Gharib School students in the Red Sea Governorate. Thesis. institute of public health , MPH, Alexandria, Egypt, University of Alexandria, High
- 72.Osman G A, Makled K M, El-Shakan Kiry HM, Metwali D M, Abd El-Aziz SS et al. (1999) Coccidian parasites as a cause of watery diarrhea among protein energy, Malnourished and other immunocompromised Egyptian children J Egypt Soc Parasitol;. 29(3), 653-68.
- 73. (2007) Virtual center of environmental technology exchange Cryptosporidium control in drinking water. Available* from: Copyright ©. all right reserved , Japan
- 74.Fayad I, Kamel M, Abou Zikri M, Hasan M, Khashaba A. (1989) Cryptosporidiosis: Etiology agent of acute diarrhea in Egyptian children. , Egypt J pediatr 6(12), 23-9.
- 75.Aboul-Magd L A, Abou Shady O. (1986) A preliminary study of human cryptosporidiosis. , J Egypt Soc Parasitol; 16, 573-7.
- 76.Menorca D M, loxer M A, Al Cantara AK, Javato-Laxer M, Fernando M T.Ganzales V(1994). Statistical analysis of clinical, immunological and nutritional factors in pediatric cryptosporidiosis in the Philippines. Southest Asian J Trop Med. Public Health;. 25, 300-4.
- 77.Katsumata T, Hosea D, wasito E B, Kohno S, Sowparto P Harak et al. (1998) Cryptosporidiosis in Indonesia: a hospital based study and a community based survey. Am j Trop Med Hyg;. 54(4), 628-32.
- 78.WHO. (1987) Prevention and control of intestinal parasitic infections report of WHO Expect committee, Geneva; Tech Rep ser No:. 749.
- 79.S Mc Carthy J, Peacock D, Trown K P. (2002) Endemic invasive amoebiasis in northern Australia. , Med J Aust; 177, 270.
- 80.Gupta S C, Gupta A K, Keswani N K, Singh P A, Tripathi A K et al. (1989) Pathology of tropical appendicitis. , J Clin Path India; 42(11), 1169-72.
- 81.Cerva L, Schrottenbaum M, Kliment V. (1991) Intestianl parasites: a study of human appendices. 38(1), 5-9.
- 82.EL- Sahn AA, El Daly SM, Elsahn F F, Soliman N K, Omar E A et al. (1992) Study of some factors related Giardia lamblia infected children. Bulletin of high institute of public health;. 32, 499-513.
- 83.Roche J, Benito A. (1999) Prevalence of intestinal parasites ifnecitons with special reference toEntameba histolyticaon the island of Bioko Equatorial Guinea. , AM J Trop Med Hyg 60, 257-62.
- 84.Sallon S, R El Shawwa, Khalil M, J Ginshurg G El-Tayib, El-Eila F.et al.,(1994). Diarrhoeal disease in children in Gaza. Ann Trop Med parasitol;. 88, 175-82.
- 85.Du Pont HL, Backer H D. (1995) Infectious diarrhea from wilderness and foreign travel. In Auer back PS, ed. Wilderness medicine: management of wilderness and environmental emergencies 3, 1028-9.
- 86.Goldmann D A, Wilson C M. (1997) Pin worm infestations in Hoekelman RA, Prim Pediatr Care. 3, 1519.
- 88.Sarmast M H, Marghi S, Elahi A, mostafi N E. (2005) Evaluationofappendicitis duetoEnterobius vermiculeris.21(2): 202-5.Pak J Med Sci.
- 89.Al Rabiah F, Halim M A, Ellis M E, Abdulkareem A. (1996) vermicularisand A cute appendicitis. , Saudi Med J; 17, 799-802.
- 90.Budd J S, Armstrong C. (1987) Role ofEnterobius vermicularisin. , Etiology of appendicitis.Br J Surge; 74, 748-9.
- 91.Mj Area, Gates R A, Groner J I, Hammond S, Caniano D A. (2004) Clinical manifestation of appendiceal Pin worms in children: an institutional experience and a review of literature;. 20(5), 372-5.
- 92.Okaya P, Ertug S. (2004) Intestinal parasites prevalence and related factors in school children, a western city sample Turkey. , BMC Public Health 4, 64-70.
- 93.Soliman N F, El Daly SM, Bassiouny H K. (1992) Strongyloides stercoralis infection among school children in rural areas in Alexandria. , Bulletin of High Institute of Public Health; 22, 619-35.
- 94.Dorfman S, Cardozo J, Dorfman D, Delvillar A. (2003) The role of parasites in acute appendicitis of pediatric patients. 44(4), 337-40.
- 95.El-Gindy M S, Morsy T, Bebars M A, Sarwat A M, El-Missiry A et al. (1986) Parasitic infection in school students in Suez Canal zone with the possible immunological changes. , J Egypt. Soc Parasitol; 16, 661-75.
- 96.El Sahly AM, Zakaria S, Ahmed L, Mabrouk M A, Thakeb F et al. (1990) Intestianl helminthic and protozoal infections and urinary schistosomiasis in Egyptian children. , J Egypt Soc Parasitol; 20, 9-21.
- 97.H El Tawil. (2001) Irnrnunoparasitological study on common intestinal protozoal infection among school students. DPH thesis. High Institute of public Health. , Alexandria University
- 98.Abdel-Hafez K. (2003) Prevalence of skin diseases in rural areas of Assiut Governorate, Upper Egypt. , Int J Dermatol 42(11), 887-92.
- 99.Shubair M E, Yassin M M, Al, AL Wahaidi AA, Fadallah S Y et al. (2000) Intestinal parasites in relation to haemoglobin level and nutritional status of school children in Gaza. , J Egypt Soc Parasitol; 30(2), 365-75.
Cited by (14)
This article has been cited by 14 scholarly works according to:
Citing Articles:
BMC Public Health (2025) OpenAlex Semantic Scholar Crossref
Cureus (2025) Crossref
Deleted Journal (2024) OpenAlex
Gut Pathogens (2024) OpenAlex Semantic Scholar Crossref
Journal of Parasitology Research (2024) OpenAlex Semantic Scholar Crossref
Bionatura (2023) OpenAlex Semantic Scholar Crossref
Journal of Desert and Environmental Agriculture (2021) OpenAlex Semantic Scholar
PLoS neglected tropical diseases (2021) OpenAlex Semantic Scholar Crossref
PLoS ONE (2021) OpenAlex Semantic Scholar Crossref
Research Square (Research Square) (2020) OpenAlex
Open Journal of Ecology (2020) OpenAlex Semantic Scholar Crossref
International Journal of Current Microbiology and Applied Sciences (2020) OpenAlex Semantic Scholar
Journal of the Egyptian Society of Parasitology (2019) OpenAlex Semantic Scholar
International Journal of Aquaculture Research and Development (2019) OpenAlex Crossref