Strengthening TB Infection Control and Its Impact on TB Screening Practices Among Healthcare Workers During The COVID-19 Pandemic in Zimbabwe
Abstract
Introduction
The risk of exposure to M. tuberculosis among healthcare workers (HCW) remains a public health concern worldwide. During the COVID-19 pandemic, the Biomedical Research and Training Institute supported the Zimbabwe Ministry of Health and Child Care in strengthening infection prevention and control (IPC) practices in healthcare facilities (HCF), integrating tuberculosis (TB) infection control (TBIC) into the intervention strategy. We describe the impact of this intervention on TBIC practices and HCW screening outcomes.
Methods
The strategy, implemented from June 2021–September 2022, included IPC mentorship training, competency assessments, and use of a standardized risk assessment tool for progress monitoring. For the training purposes, the project developed eight practical problem-solving IPC modules including an occupational health component. Trained mentors conducted bi-monthly site support visits (SSV), used a checklist to track compliance, and assessed competencies of HCW at the targeted facilities. Facility-based risk assessments were conducted three times during the project implementation.
Results
During the intervention, 1,865 HCW from 105 facilities were trained. Availability and use of personal protective equipment improved by 49% and 42%, respectively. The proportion of HCF with designated areas for sputum collection increased by 43%. The proportion of HCF that screened HCW for TB increased by 42% with 3,761 HCW screened during the project period. Fourteen were diagnosed with TB and referred for care, resulting in 372 new cases per 100,000.
Conclusion
The implemented strategy of training, mentorship, and regular SSV strengthened TBIC measures, improved TB screening practices and case finding among HCW. Improving and maintaining practices is critical for effective TBIC.
Article Information
- Received
- Accepted
- Published
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Alethea Mashamba, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Julia Ershova, U.S. Centers for Disease Control and Prevention, Atlanta, Georgia, United States of America —
Competing Interests
The author declares no conflict of interest.
Funding
Funding for this evaluation was provided by the Coronavirus Aid, Relief, and Economic Security Act (CARES-ACT) through the US Centers for Disease Control and Prevention (CDC) under grant # 6 NU2GGH001936-05-08.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
The authors would like to express gratitude to health facility administration and staff throughout Zimbabwe, members of the BRTI and ICAZ-T teams, the HATIPP-ZIM Directorate of Nursing, and the Zimbabwe Ministry of Health and Childcare.
Citation:
Introduction
Globally, tuberculosis (TB) is the leading cause of death from a single infectious agent, M. tuberculosis (MTB). A total of 1.23 million people died from TB in 2024 1. Health care workers (HCW) are on the front lines of patient care, and their exposure to infectious agents, including MTB, can lead to significant consequences, including the development of active disease, which can result in prolonged illness, increased healthcare costs, and potential transmission to patients and colleagues. Reducing the risk of HCW exposure to MTB is a critical challenge that must be addressed across all healthcare settings 2, 3, 4. To maintain sustained safe and quality service delivery, it is critical to ensure continuous and improved infection prevention and control (IPC) measures that are broad-based and cover various infectious diseases, including TB 5.
Zimbabwe has historically had a high burden of TB and is on the global list of 30 high-burden TB countries and has an estimated TB incidence as high as 203 per 100,000 population 1. Of note, the country was temporary removed from this list in 2021, as the estimated incidence of TB decreased from 242 per 100,000 in 2015 to 199 per 100,000 in 2019 6. The COVID-19 pandemic disrupted TB care services as a result of many reasons, including supply chain interruptions leading to reduced IPC supplies (such as personal protective equipment (PPE)), COVID-19 infections among HCW, government mandates to change some facilities from general purpose to COVID-specific facilities, reductions in clinic appointments due to social distancing requirements, etc. 7. During the pandemic, the estimated TB incidence in Zimbabwe rose to 204 per 100,000 in 2022 and further to 211 per 100,000 in 2023, resulting in Zimbabwe being reinstated on the Global list of 30 high-burden TB/HIV and MDR/RR-TB countries 1. TB infection continues to be a significant problem in Zimbabwe, and HCW remain at risk of work-related exposure to MTB 8, 9.
TB infection control has always been a part of the Zimbabwe National IPC training program which was re-established in 2012 with support from BRTI and ICAZ-T, and funding from the U.S. President's Emergency Plan for AIDS Relief (PEPFAR) through the U.S. Centers for Disease Control and Prevention (CDC) during Zimbabwe Infection Prevention and Control Project (ZIPCOP, 2012-2017) 10, 11. In 2017, the Healthcare Associated TB Infection Prevention Project (HATIPP-Zim) was initiated to support MoHCC in preventing healthcare-associated TB infection in Zimbabwe. The central focus of HATIPP-Zim was to support TB screening and treatment in HCW. Following the project objectives, an intervention for improving TBIC practices was conducted in 104 healthcare facilities in 2017-2019 12. A draft National TB-HCW screening policy was developed, and a screening program among HCW was established. Data collected in 2018 from these targeted facilities showed a high incidence of TB among HCW (528/100,000), highlighting the need to improve and maintain the TBIC practices, including a TB screening program among HCW 13.
During the COVID-19 pandemic, the Biomedical Research and Training Institute (BRTI), in collaboration with the Infection Prevention and Control Association Trust (ICAZ-T), assisted the Zimbabwe Ministry of Health and Child Care (MoHCC) in enhancing IPC practices across 105 healthcare facilities in Zimbabwe. The global and the MoHCC guidelines on IPC recommend administrative, environmental, and respiratory protection measures to reduce the risk of respiratory pathogens transmission in healthcare settings 2, 13, 14, 15. Prevention of healthcare-associated transmission of infectious diseases is dependent upon sustained and integrated interventions for improvement of IPC measures. These interventions are crucial for early detection and treatment of TB among HCW, thereby reducing the risk of transmission within healthcare settings 2, 16, 17. The goal of the current intervention was to strengthen TB Infection Control (TBIC) measures during the COVID-19 pandemic, including TB screening practices and outcomes among HCW 18. We therefore aimed to evaluatethe impact of these interventions on TBIC practices and HCW screening outcomes in the targeted healthcare facilities, emphasizing the importance of maintaining a safe healthcare environment for both workers and patients.
Methods
This was a quasi-experimental before–after study without a control group, based on repeated facility-level assessments conducted over the project period.
From June 2021 to September 2022, an intervention to strengthen IPC measures for respiratory diseases, including COVID-19 and TB, was implemented in 105 health facilities in four rural provinces (Mashonaland East, West, Central, and Matabeleland North) and the municipal province of Harare (Figure 1). The selected facilities comprised 66 primary and 39 secondary HCFs from 25 districts (Supplementary Table S1). The criteria used for selection of the facilities included a high number of COVID-19 cases, inadequate training in IPC/TBIC resulting in poor performance, severe staff shortages, and geographic remoteness of the facilities 2, 18, 19, 20, 21.
The implementation of an IPC programme at a health facility requires the appointment and training of an IPC focal person (IPCFP) with defined roles and responsibilities, and with dedicated time to carry out IPC activities, as well as appropriate training of all HCWs. For the intervention strategy, we appointed 70 IPC mentors across all districts (“the mentors” hereafter), who were capacitated to roll out the strategy in the selected facilities. The mentors attended a series of blended trainings, including virtual sessions via Zoom and face-to-face sessions, followed by ongoing support from the project team through WhatsApp messaging. For training in TBIC and the TB screening protocol for HCWs, training materials and the draft National Policy on TB Screening of Healthcare Workers developed during the HATTIP-ZIM project were used.
The training materials were based on guidance from the World Health Organization (WHO) IPC Assessment Framework (IPCAF) and the TB Building and Strengthening Infection Control Strategies (TB BASICS), a framework developed by the U.S. CDC to support facility-level assessment, planning, and continuous improvement of TB IPC practices 15, 22, 23. IPC training and ongoing mentorship are key components of this framework to promote capacity building and sustainability 16, 24, 25. Competency assessments in hand hygiene, donning and doffing of PPE (including surgical masks and N95 respirators), and environmental cleaning complemented the training programme (Supplementary Forms S1–S3). Training registers and mentorship reports were used to document and monitor these activities (Supplementary Form S4).
Figure 1. Map of Zimbabwe with the five provinces with interventions highlighted. 
Download figure
To monitor progress in strengthening IPC and TBIC programmes in clinics and hospitals, mentors were trained to use a standardized IPC risk assessment tool (Supplementary Forms S5–S6). The tool was developed based on national IPC guidelines and IPCAF and adapted to the local setting using the TB BASICS template. It was designed to promote standardization by using objective measures for evaluating IPC indicators wherever possible. Risk assessments were conducted at the start of the project and during two subsequent follow-up visits, and the results were reported to District and Provincial Health Executives.
Although exposure of HCWs to COVID-19 was a major focus during the project period, concerns about TB exposure led to the inclusion of additional TB-related indicators to monitor TBIC implementation. Initially, 19 IPC indicators were reported monthly to track compliance with recommended COVID-19 and TBIC practices 15, 26. In 2022, 13 TB-specific indicators (e.g., number of HCWs screened for TB and number of new confirmed TB diagnoses among HCWs) were added to the reporting following increased concern about TB exposure (Supplementary Table S2).
District mentors were responsible for compiling and entering data into KOBOCOLLECT software, which was used for data collection and analysis and installed on tablets provided to the mentors 27. The BRTI/ICAZ-T project team monitored data collection through regular data quality assessments. TB-related indicators included the number of facilities implementing TBIC training for HCWs, the presence of TB screening integrated with COVID-19 screening, and the availability and appropriate use of surgical masks and N95 respirators. Mentors conducted bi-monthly site support visits (SSVs) using an indicator checklist to track compliance with IPC requirements to prevent COVID-19 and TB transmission in healthcare facilities and reported findings to provincial managers on a quarterly basis (Supplementary Forms S6–S7).
In addition, eight practical problem-solving IPC training modules, including an occupational health component, were developed and used by mentors to reinforce TBIC practices and HCW screening during SSVs and training sessions conducted at District Health Management meetings. The purpose of the modules was to support HCWs in the on-site implementation of IPC measures, focusing on key standard precautions to prevent the transmission of infections in HCFs. The modules were pilot-tested in Harare municipal clinics, and a user manual was developed to guide their use.
To evaluate the impact of the implemented measures on TBIC performance in the participating facilities, facility-level performance was assessed using quantifiable indicators for IPC core components and administrative, environmental, and respiratory protection controls at the start of the project and during two follow-up visits. As the number of facilities assessed differed between time points, proportions were compared using the chi-square test for independent samples, with a two-sided p-value < 0.05 considered statistically significant.
Results
Over the project period, assessments of HCFs were conducted quarterly. The number of assessed facilities varied by quarter, ranging from 83 in the first assessment (Q3 2021) to 105 in the final quarter (Q3 2022) (Table 1).
At the project initiation, 90% (75/83) of facilities had screening and triage processes in place, increasing to 100% (105/105) by the end of the project (p = 0.013) (Table 1). The proportion of facilities receiving training and educational materials on screening and triage, as well as those with written procedures in place, also increased significantly over the project period (p < 0.0001) (Table 1).
The proportion of facilities with a trained IPC focal person (IPCFP) increased from 87% (72/83) at the start of the project to 94% (99/105) by the end of the project, although this difference was not statistically significant (p = 0.073) (Table 1). While all targeted facilities in Mashonaland Central and East provinces had a trained IPCFP in place, lower coverage was observed in Harare, Mashonaland West, and Matabeleland North provinces, reflecting high staff attrition in these areas.
Staff shortages were reported throughout the project period. As the COVID-19 pandemic evolved, increased staff attrition limited the ability of facilities to dedicate clinical staff to screening and triage activities. To address this, facilities increasingly assigned trained nurse aides to support screening and triage under clinical supervision. The proportion of facilities with staff assigned to these tasks increased by 12%, although this change was not statistically significant (p = 0.12) (Table 1).
Table 1. Progress in strengthening IPC program in selected health facilities across five provinces in Zimbabwe, June 2021–September 2022| Q3_2021 | Q4_2021 | Q1_2022 | Q2_2022 | Q3_2022 | ||
| Number of facilities assessed | 83 | 58 | 84 | 105 | 105 | |
| Indicator | % (n) | % (n) | % (n) | % (n) | % (n) | p-value * |
| Proportion of HCFs that have screening and triaging of patients with respiratory symptoms in place. | 90% (75) | 97% (56) | 97% (81) | 98% (103) | 100% (105) | 0.013 |
| Proportion of HCFs that received training and educational materials on screening and triaging of patients with respiratory symptoms | 80% (66) | 81% (47) | 90% (76) | 98% (103) | 99% (104) | <0.0001 |
| Proportion of HCFs with developed and approved written procedures for screening and triaging of patients with respiratory symptoms. | 58% (48) | 79% (46) | 92% (77) | 87% (91) | 92% (97) | <0.0001 |
| Proportion of HCFs with an IPCFP in place. | 87% (72) | 95% (55) | 93% (78) | 94% (99) | 94% (99) | 0.073 |
| Proportion of HCFs that have designated staff to screen and triage patients. | 76% (63) | 64% (37) | 75% (63) | 85% (89) | 85% (89) | 0.12 |
Capacity building activities were associated with improvements in TB infection control (TBIC) practices. The proportion of facilities receiving TBIC training increased from 75% (63/84) to 99% (104/105), p<0.0001, and a total of 1,865 healthcare workers (HCWs) were trained. The proportion of facilities screening HCWs for TB increased from 52% (44/84) to 74% (78/105), p=0.003 (Table 2). Facilities that were screening HCWs for TB at the start of the project continued this practice, building on training provided during the previous HATTIP-Zim project.
During the project period, 3,761 HCWs were screened for TB, of whom 14 were diagnosed with TB and referred for care, corresponding to 372 cases per 100,000 HCWs screened. At the beginning of 2022, 52% (44/84) of facilities had designated areas for sputum collection. Following TBIC refresher training, this proportion increased to 97% (102/105), p<0.0001 (Table 2).
Table 2. Improvement in TB-related IPC practices in selected health facilities across five provinces in Zimbabwe, January-September 2022.| Q1_2022 | Q2_2022 | Q3_2022 | ||
| Number of facilities assessed | 84 | 105 | 105 | |
| Indicator | % (n) | % (n) | % (n) | p-value * |
| Proportion of facilities that received training in TBIC in the last year | 75% (63) | 84% (88) | 99% (104) | <0.0001 |
| Proportion of Facilities that are Screening HCW for TB | 52% (44) | 62% (65) | 74% (78) | 0.003 |
| Proportion of Facilities with designated sputum collection area (outside the HCF) | 52% (44) | 89% (93) | 97% (102) | <0.0001 |
Improvements in IPC practices were further supported by supportive supervision and mentorship. Availability and appropriate use of personal protective equipment, including N95 respirators, increased substantially during the project period (Figure 2), with significant improvements observed in both availability and correct use (p < 0.0001).
Figure 2. Availability of N95 Respirators and improved competence in donning and doffing in health facilities across five provinces in Zimbabwe, January-September 2022.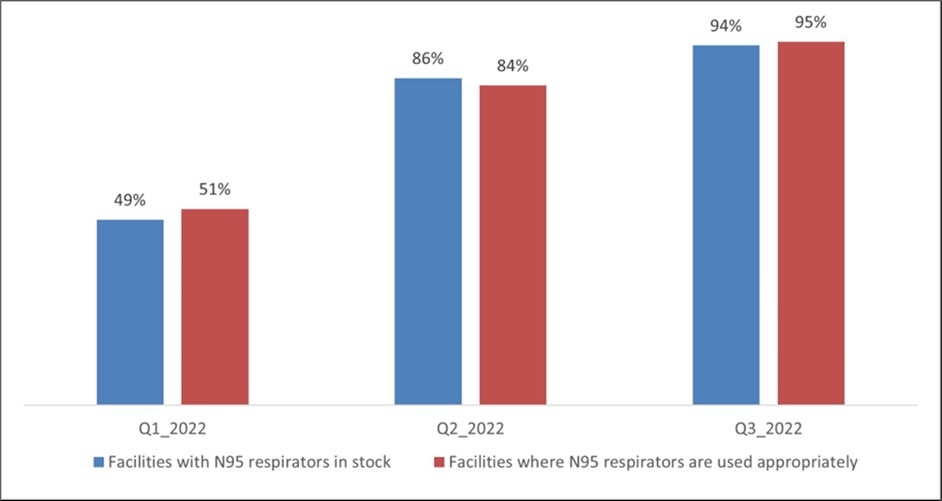
Download figure
Discussion
Our intervention to strengthen IPC during the COVID-19 pandemic was associated with improvements in TBIC practices across participating facilities. These findings suggest that integrated approaches combining training, mentorship, and supportive supervision can enhance implementation of TBIC measures, even in the context of health system strain during a public health emergency. Strengthening healthcare worker capacity and reinforcing routine screening practices are particularly important for reducing the risk of TB transmission in high-burden settings.
The TB BASICS model, upon which this intervention is based, has been implemented in 18 countries around the world. In Zambia and Botswana, facility assessments showed an increase in IPC performance scores and notable improvements in triage and fast-tracking of coughing patients, active TB screening, and provision of N95 respirators 28, 29.TB IPC policies and practices improved following implementation of TB BASICS in China in 2017-2019 30, 31. The training component of TB BASICS helped to increase the capacity of healthcare professionals to manage TB transmission risks in the covered facilities in China. The "TB Mukt Bharat (TB Free-India) Infection Prevention and Control" project in India used the mentorship models, training curricula and tools developed by TB BASICS initiative to build the capacity of healthcare facilities and achieve IPC compliance 32. Key indicators of IPC interventions increased significantly after one year of implementation of TB Mukt Bharat IPC activities. Implementation of the TB BASICS initiative in Nigeria resulted in substantial improvement in managerial, administrative, environmental, and personal protective measures and in demonstrable country and facility commitment to the initiative during a 6-month implementation period 22. The incidental diagnoses of TB among health care workers as a result of this project highlight the value of routine health care worker screening and underscore the importance of TB infection control in health care settings of the country.
During the intervention period, a large number of HCW were trained in Zimbabwe. As a result, appropriate use of PPE (N95 respirators) was greatly improved. Further, the proportion of HCF that screened HCW for TB also increased during the project period. However, TB incidence among HCW remains high, outlining the importance of further measures for preventing the TB transmission in healthcare settings. The effectiveness of IPC interventions in reducing transmission of MTB among HCW has been estimated in several studies 33, 34. Although the TB incidence among HCW in our study was lower than that reported in previous studies, which have demonstrated elevated TB incidence among HCWs in high-burden settings, this difference cannot be attributed to the intervention 2, 13, 35.
The findings from the project implementation led to thorough review and update of Zimbabwe’s National IPC Policy which was signed by the MoHCC in the fall of 2024 36, 37. The updated policy includes a requirement for a HCW surveillance system to be put in place, including TB screening at the start of employment, annually or bi-annually as per risk, and out of cycle. IPC reporting indicators were enhanced by including the number of HCW who developed TB. Data on the IPC indicators are to be collected on quarterly basis and reported to the Health Information System. A budgeted National IPC Strategic Plan has been developed to implement the updated National IPC Policy 38. Furthermore, a Monitoring and Evaluation Plan, along with an IPC Strategic Plan performance framework, were developed to monitor the outputs of the program 39. In addition, the administrative and reporting structure of the IPC program at District, Provincial and National level was clearly defined according to the observations during the intervention.
This study has several limitations. First, the number of facilities assessed differed across time points, which limited the ability to conduct paired analyses and may have introduced selection bias. Second, high attrition of healthcare workers during the COVID-19 pandemic may have affected the continuity of IPC implementation and the availability of trained IPC focal persons, potentially influencing observed outcomes. Third, the use of facility-level indicators may not fully capture the quality or consistency of IPC practices, and improvements may partly reflect reporting rather than actual changes in practice. Fourth, the use of digital platforms such as WhatsApp for ongoing support may have resulted in differential access to the intervention, as facilities or healthcare workers with limited connectivity or access to mobile devices may have been less able to participate fully, potentially introducing bias. Finally, the observational design without a control group limits the ability to attribute changes solely to the intervention.
Conclusion
Despite the limitations, our results highlight the importance of improving IPC through consistent training and implementation of IPC measures to protect HCW from occupationally acquired respiratory infections such as TB. Our findings also demonstrate that HCW are still at risk of work-related TB, and therefore sustained TBIC measures and robust surveillance systems for monitoring TB among HCW are critical beyond the COVID-19 pandemic. All healthcare programs could benefit from implementing, improving and maintaining practices for TBIC.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funding agencies.
Ethical Approval
This project was reviewed by the BRTI Institutional Review Board (BRTI-IRB) and exempted from Full Committee Review as the project does not constitute human subject research. The project was also reviewed by CDC, deemed not research, and was conducted consistent with the applicable federal law and CDC policy. The study was conducted in accordance with the Declaration of Helsinki.
Supplementary Material
References
- 2. (2019) World Health Organization. WHO guidelines on tuberculosis infection prevention and control. , Geneva:
- 3.Joshi R, Reingold A L, Menzies D, Pai M. (2006) Tuberculosis among health-care workers in low- and middle-income countries: a systematic review.PLoSMed. 3-12.
- 4.Baussano I, Nunn P, Williams B, Pivetta E, Bugiani M et al. (2011) Tuberculosis among health care workers.Emerg Infect Dis. 17(3), 488-494.
- 5.Allegranzi B, Nejad S B, Combescure C. (2011) Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis.Lancet. 377(9761), 228-241.
- 7.CRS Mackworth-Young, Chingono R, Mavodza C. (2021) . Community perspectives on the COVID-19 response, Zimbabwe.Bull World Health Organ 99(2), 85-91.
- 8.Centers for (2025) Disease Control and Prevention. HIV and TB overview: , Zimbabwe. Atlanta: CDC; .
- 9. (2021) Ministry of Health and Child Care (Zimbabwe).National health strategy for Zimbabwe 2021–2025. , Harare: MoHCC;
- 10.Robertson V, Maruta A, Mashamba A. (2014) A national infection prevention and control training strategy in Zimbabwe: rewards and challenges. ICAN Conference;. , Harare, Zimbabwe
- 11.S U. United States Department (2012) and Zimbabwe partner to improve infection control practices in health care facilities.
- 12.Team HATIPP-ZIM. (2019) Healthcare-associated tuberculosis infection prevention project (HATIPP-ZIM) 2016–2019 report. , Harare: MoHCC;
- 13.Mutsvangwa J. (2016) Measuring progress of TBIC implementation in health facilities and TB screening among healthcare workers. 6th ICAN Congress;. , Johannesburg, South Africa
- 14.Jensen P A, Lambert L A, Iademarco M F, Ridzon R. (2005) Guidelines for preventing the transmission ofMycobacterium tuberculosisin health-care settings. 54(17), 1-141.
- 16.Health World. (2016) Organization. Guidelines on core components of infection prevention and control programmes. , Geneva: WHO;
- 17.Gozdzielewska L. (2024) Interventions for preventing or controlling healthcare-associated infections: a scoping review.Am J Infect Control.
- 18.Health World. (2021) Organization. Infection prevention and control during health care when COVID-19 is suspected or confirmed. , Geneva: WHO;
- 19.Health World. (2022) Organization. Maintaining infection prevention and control measures for COVID-19 in health care facilities. , Geneva: WHO;
- 20.Murewanhema G. (2022) Public health sector capacity and resilience building in Zimbabwe: an urgent priority.SAfrMed J. 112-4.
- 21.Kavenga F, Rickman H M, Chingono R. (2021) Comprehensive occupational health services for healthcare workers in Zimbabwe during the SARS-CoV-2 pandemic.PLoSOne. 16-0260261.
- 22.Dokubo E K, Odume B, Lipke V. (2015) Building and strengthening infection control strategies to prevent tuberculosis —. , Nigeria 65-10.
- 23.O'Connor S, Ali H. (2025) TB BASICS: a framework to improve infection prevention and control. 65(4), 2500382-10.
- 24.Storr J, Twyman A, Zingg W. (2017) Core components for effective IPC programmes.AntimicrobResist Infect Control. 6, 6.
- 25.Health World. (2018) Organization. Advanced infection prevention and control training: leadership and programme management module. , Geneva: WHO;
- 26.Health World. (2020) Organization. Infection prevention and control health-care facility response for COVID-19. , Geneva: WHO;
- 28.Moshe Y, Garekwe M, Jibril H B. (2013) Continuous quality improvement approach to TB infection control. 44th Union World Conference on Lung Health; , Paris, France .
- 29.Emerson C, Lipke V, Kapata N. (2016) Evaluation of TB infection control implementation.Int JTubercLung Dis. 20, 941-947.
- 30.Zhang C, O'Connor S, Smith-Jeffcoat S E. (2024) Implementing a continuous quality-improvement framework for TB IPC.Infect Control HospEpidemiol. 45(5), 651-657.
- 31.Zhang C, O'Connor S, Chen H. (2025) . Indicator-based TB IPC assessments in China.Am J Infect Control 53(4), 506-513.
- 33.Karat A S, Gregg M, Barton H E. (2020) Triage and respiratory isolation to reduce TB transmission.Clin Infect Dis. 720.
- 34.Azeredo A C, Holler S R, de Almeida EG. (2020) Tuberculosis in health care workers and infection-control measures.Workplace Health Saf. 68(11), 519-525.
- 35.da Silva EH, ERN Lima, dos Santos TR, Padoveze M C. (2022) Prevalence and incidence of tuberculosis in health workers.Am J Infect Control. 50(7), 820-827.
- 36.Ministry of Health, Care Child. (2024) . Zimbabwe National Infection Prevention and Control Policy and Strategic Plan , Harare: MoHCC; .