
Rehabilitation With Corticobasal and Compressive Implants with Polished Surface in Case of Failure with Two Stage Implants-Article
Abstract
The aim of this article is to present alternative possibilities for corrective intervention using corticobasal implants, following the failure of treatment with two stage implant in cases of extensive edentulism, multi-segmented edentulism, and the development of peri-implantitis 1 at the level of these implants. For this purpose, a case was selected involving a patient treated with two stage implants in a multi-segmented manner, in the distal regions of the maxilla and mandible, where the implants were affected after 12 years by peri-implantitis in proportions ranging from 20% to 100% in different areas of bone, with a predominance in the vestibular area. The decision was made to remove the affected two stage implants, as well as the remaining deciduous teeth, with or without periodontal conditions, but whose position on the arch made improperly rehabilitation, both functionally and aesthetically impossible, and made the second rehabilitation with polished corticobasal and compressive implants in immediate loading 2. Function and aesthetics of the gnathological apparatus were restored through definitive fixed metal-ceramic prosthetics on the support of corticobasal and compressive implants within 4 days from the beginning of the treatment, with the result being monitored over a period of 3 years and 3 months, and this evaluation is to continue over time. From a surgical perspective, for secondary rehabilitation with polished corticobasal and compressive implants, strategic positions in the maxillary and mandibular bones were used as follows: the fusion area of the maxillary bone with the sphenoid bone, the nasal cortex, the sinus cortex the lingual cortex distal to the mylohyoid line, and the interforaminal mandible area.3, 4 These areas correspond to methods described in Consensus Number 6 in the IF The Foundation of Knowledge 5. In conclusion, the treatment with corticobasal, compressive polished implants is successful even in the case of a difficult clinical scenario like the one described for this patient 6. The reduced treatment time, along with the absence of the need for sinus lifts or bone grafts, makes it the ideal solution in any situation. The use of corticobasal implants, with fixation in the second/third cortical layer and an immediate loading protocol, should represent the primary solution in treating cases with poor bone representation, and no only as a “Corrective Intervention with Corticobasal® Implants”7.
Article Information
- Received
- Accepted
- Published
Academic Editor: Sasho Stoleski, Institute of Occupational Health of R. Macedonia, WHO CC and Ga2len CC
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Fodor Romulus Calin.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Fodor Romulus Calin, Dr. Fodor Romulus Calin’s Clinic of Dentistry and Implantology, Str. Dragoş Vodă 8, 405300 Gherla, Romania; Implant Foundation Teacher -www.implantfoundation.org —
Competing Interests
The authors declare no conflicts of interest.
Funding
“This research received no external funding”
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
The popularity of two stage dental implants is largely due to their use in simple cases with sufficient bone, by practitioners who do not require special training, and them presentation in university courses as a universal panacea. However, these implants are increasingly being used in more complex cases where native bones are insufficient, requiring bone grafts and sinus lifts, which ultimately results in a significantly higher failure rate 8. When we talk about failure, we’re not only referring to what will happen years later due to peri-implantitis, but also to immediate failures, such as those arising from complications due to bone grafting and/or sinus lift surgeries, or from patients abandoning treatment before completing the prosthetic work on the implants between these stages. The advantage of immediate loading on implants specifically prevents this last failure—the non-completion of the prosthetic work—and the use of corticobasal implants addresses the primary failures identified. It is well known that there is a direct correlation between the occurrence of peri-implantitis and the implant surface – the mechanically and chemically treated surface that becomes exposed to the oral cavity. Additional factors include: the large diameter of the implant, the junction between the endosseous implant and the prosthetic component, occlusion – without excluding other causes. On the other hand, there are doctors who claim that treatment with corticobasal implants lack a scientific foundation that would make it universally accepted treatment in the field of implant rehabilitation. What is insufficiently connected to the treatment with corticobasal implants is the acceptance and teaching of these treatments at the university level, not the lack of scientific evidence, evidence which can be consulted in books and articles. The treatment with multifaceted implants with mechanic and chemical treated surfaces has the following disadvantages that lead to peri-implantitis: -loss of contact between the implant and the crestal bone due to the continuous physiological remodelling of the bone under the influence of masticatory forces (Wolff's law).
-large diameters that, in cases of bone atrophy, lead to placement too vestibular, towards the less represented cortical bone, resulting in implant exposure.
-implant fixation in reduced native bone, requiring sinus lift and bone augmentation in the maxillary area.
-insufficient number of implants to transmit occlusal forces to the cranial lines of force.
-insufficient distal implants to prevent distal cantilever.
Treatment with corticobasal implants needs:
-a larger number of implants, primarily due to the need for immediate loading with definitive fixed restorations, but also because of anchorage in native bone, which inmany cases are deficient.
-in segmental restorations, the need to sacrifice certain teeth located in areas that must
be accessed with corticobasal implants 9.
-in the event of failure, a second rehabilitation is possible within the same timeframeand with the same cortical fixation technique as in the initial rehabilitation.
The treatment with any type of implants may be compromised under the followingconditions:
-remaining of natural teeth affected by periodontal diseases.
-remaining of natural teeth with positional deficiencies that prevent the establishment ofa correct occlusion.
-remaining of natural teeth that hinder access to native bone areas in strategic positionsin cases of severe atrophy.
Under these conditions, to choose for treatment with corticobasal and/or compressiveimplants with mechanically polished surfaces can reduce peri-implantitis to near zero.Treatment with corticobasal implants requires different knowledge of applicabilitycompared with two stage implants, and additional training for the clinician in this fieldis necessary to optimally utilize this new technology. The existence of well-definedprotocols and organized educational structures in many countries make thistreatment accessible to physicians in favor of patients.
For the patient, a correct treatment with corticobasal implants, without sinus lift or boneaugmentation, shortens the waiting period for final oral rehabilitation from months oryears to 3-4 days. In cases of failure, a second rehabilitation is always possible undersimilar conditions, ensuring the patient does not remain edentulous.
Materials and Methods
Patient information: Female, 57 years old, heavy smoker (10 cigarettes/day), diagnosed with rheumatoid arthritis – medication includes Methotrexate 16 mg/day and Prednisone 8.5 mg/day. The patient is under treatment for rheumatoid arthritis with Methotrexate and Prednisone for many years. The effect of this medication on dental implants is extensively described in multiple articles, but a consensus has not yet been reached on the matter 10. Dental Implant History as Reported by the Patient (up to June 2022):
2012: Placement of 15 multiphase dental implants with bone grafting. During the course of treatment, one implant in quadrant 1 (distal) was removed prior to completion of prosthetic rehabilitation (after approximately 6 months).
2018: Patient reported masticatory pain in quadrant 3 (left posterior mandibular region).
2022: Patient underwent multiple consultations with different practitioners in order to establish a treatment plan.
June 2022: Patient presented to our clinic for immediate-loading implant treatment At the time of presentation in 06. 2022, radiologically, advanced peri- implantitis is observed around the implants, with loss of native bone in the affected distal areas (Figure 1)
Figure 1. Panoramic overview picture before rehabilitation 06.2022
Download figure
Clinically, we observe the exposure of the implants in the oral cavity with bacteria plaque on their surface, primarily due to the retentive surface of the implants. The exposure of the endosseous part of the two stage implants represents the starting point for mucositis and subsequently peri-implantitis (Figure 2). An important role is played by the occlusion of the prosthetic restorations and the way in which masticatory forces are transmitted to the implants. Prosthetic restorations with prominent vestibular cusps in contact with the opposing teeth, which during lateral movements lead to an increase in extrusive forces on the implant side (in this case, implants) (Figure 2a, b, c). A lingualized occlusion is preferred, where the masticatory forces are placed closer to the insertion axis of the implant.
Figure 2. Intraoral images of the exposed implants affected by peri-implantitis: (a) quadrant 3, vestibular view; (b) quadrant 2, vestibular view; (c) quadrant 4, vestibular view; (d) quadrant 4 after removal the prosthetic restoration and uncovering the implants, vestibulo-lingual view. 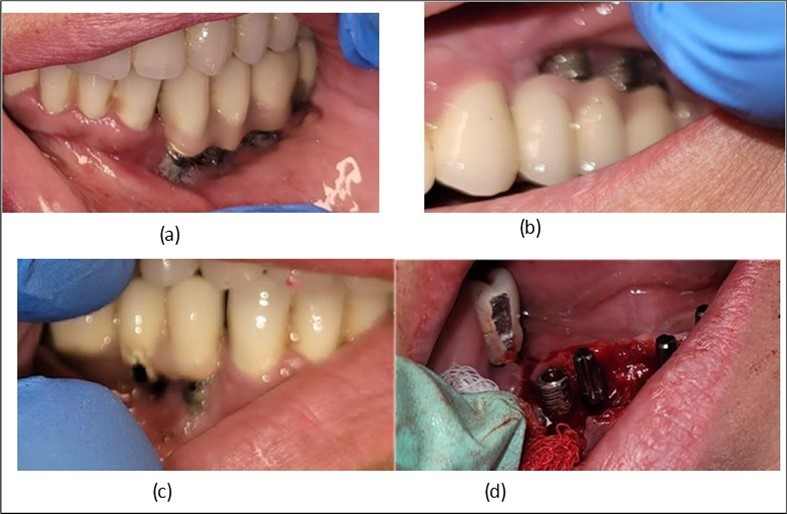
Download figure
Methodology
Plexus anesthesia is used in all working areas with Articaine 40 mg/0.01 mg/ml adrenaline. For mucosal disinfection, Betadine 10% is used.Two stage implants are removed either by simple extraction with forceps and an elevator or by using an osseous bur in cases where they cannot be easily removed using the first method. The remaining teeth are extracted, and the crest is regularized to avoid excessive future resorption, as well as to create an alveolar crest with a favourable resorption optical level for aesthetics (Figure 6, Figure 7).
In the upper anterior region, after extractions and regularization, marginal gingival connective tissue located palatine is harvested for use in augmenting the anterior area. This tissue is de-epithelized with a scalpel and kept in saline solution until used (Figure 4, Figure 5). The implants used are BCS corticobasal implants in areas with significant bone loss, and TPG compression implants, both from Dr. Ihde Dental AG, for post-extraction areas and regions with a large amount of trabecular bone but of poor quality (D3-D4). Both types of implants have a polished surface to reduce bacterial adhesion, and they feature a 2mm prosthetic collar that can be bent to parallelize the prosthetic part of the implant according to prosthetic requirements (Figure 3). The only exception to this parallelization through bending is the TPG implant in the maxillary-sphenoid fusion area (quadrant 2), were, due to lower torque, a prefabricated parallelization sleeve with a 25° angle was preferred. This sleeve was cemented before the impression was taken (Figure 3).
A total of 11 implants is placed in the maxilla, including compressive TPG implants with a polished surface in the maxillary-sphenoid fusion area (Figure 3, Figure 9). Similarly, in the anterior region, final fixation is achieved in the nasal cortex, and BCS corticobasal implants are added in areas with massive bone loss in the frontal region (Figure 3, Figure 8, Figure 11). Additionally, in the palatal sinus cortical area, with the aim of avoiding the addition and sinus lift zone where the second cortical bone no longer exists, 3 implants are placed, 2 in quadrant 1 and 1 in quadrant 2 (Figure 3, Figure 8). Through the Caldwell-Luc sinus lift procedure, the sinus cortical bone is displaced to allow the placement of the graft material and elevation of the sinus membrane. This sinus cortical is no longer recreated at the junction of the graft material and mucosa-sinus membrane, making it impossible to place a corticobasal implant, which relies on the second cortical bone. In the distal mandibular area, after the removal of two stage implants due to massive destruction in quadrant 3, implant placement distal to the mylohyoid line is not possible, as in quadrant 4 (Figure 10). A re-intervention occurs after 5 months to stabilize the area (Figure 12, Figure 14). Also, at the moment of fixation, the tip of one implant fractures, and the decision is made to leave it in place due to regional bone destruction, in order to avoid enlarging the bone defect.
In the interforaminal area (Figure 3, Figure 13), 6 corticobasal implants are also placed. The increased number of implants is due to the poorly represented distal area that needs to be compensated.
Figure 3. Panoramic pictures after removal of implants affected by peri-implantitis, extractions, alveolar crest regularization, and insertion of corticobasal and TPG implants (07.2022) 
Download figure
Considerations related to connective tissue grafting in post-extraction and post-implant defects – it is a technique that can be performed either by harvesting connective tissue from the tuberosity area, the palate, or the marginal palatal area, if the quantity is sufficient 11. It is done simultaneously with the rest of the bone regularization procedure; in this case, removal of the palatal gingival area was necessary anyway for easier cleaning and access to the frontal implants. On this occasion, after de-epithelialization, the tissue is used to restore the shape of the frontal gingival area after implant insertion (Figure 4, Figure 5).
Figure 4. Repair of the frontal area with connective tissue harvested from the marginal palatal area after extraction and crest regularization: (a) mucosal tissue piece harvested from the frontal palatal area before preparation; (b) prepared connective tissue piece placed between the frontal implants under the mobile mucosa. 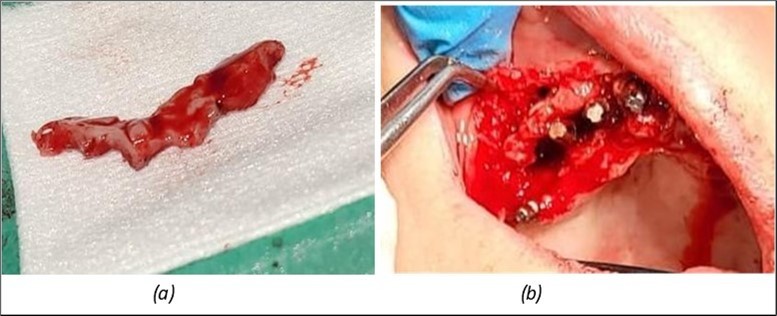
Download figure
Figure 5. Appearance of the mucosa from where the tissue was harvested and of the implants, 2 days after the corrective intervention. 
Download figure
Figure 6. Definitive metal-ceramic prosthetic restoration cemented 4 days postoperatively: (a) Junction area at the mandible between the definitive metal-ceramic prosthetic restoration and the gingiva; (b) Junction area at the maxilla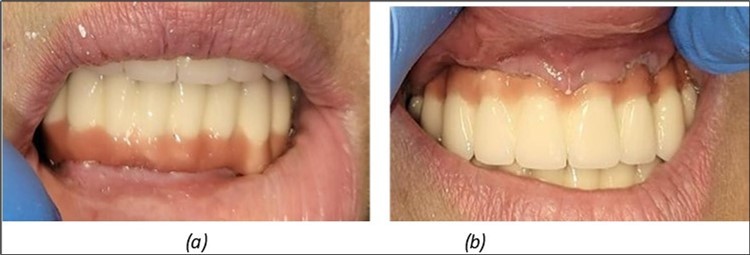
Download figure
Figure 7. (a) The aesthetic appearance of the patient from the front 4 days. b) 3 years after 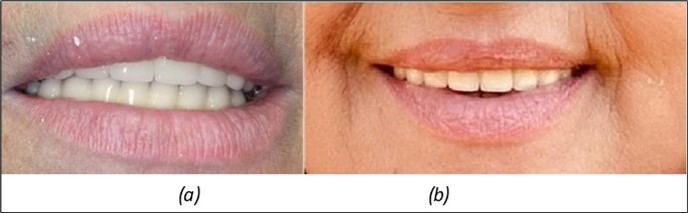
Download figure
Figure 8. (a), (b) Sinus lift and grafting area with two stage implants before their removal. (c) area of fixation of BCS and TPG implants, avoiding the sinus lift and grafting area 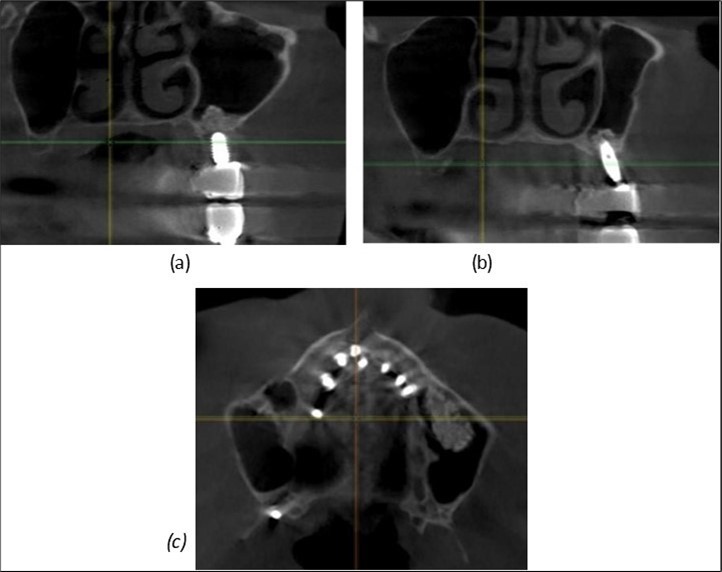
Download figure
Figure 9. Implants in the pterygoid plateau area: (a) TPG implant fixed in the maxillary-sphenoid junction area, quadrant 1; (b) TPG implant fixed in the maxillary-sphenoid junction area, quadrant 2.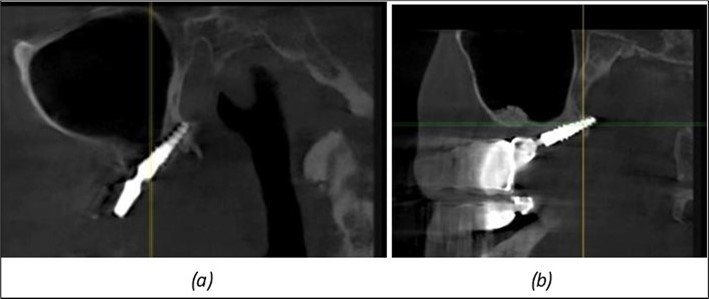
Download figure
Figure 10. Implants in the palatal sinus cortical area to avoid bone grafting: (a) BCS implant partially fixed in the graft material mass, partially in the palatal cortex; (b) Implant fixed in the palatal cortex at the junction with the nasal cortex, behind the graft material mass. 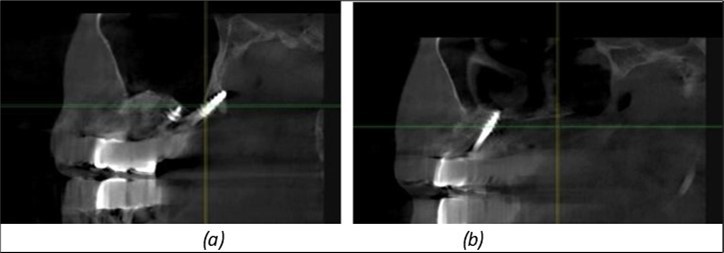
Download figure
Figure 11. Implants in the anterior area anchored in the nasal cortex (BCS and TPG): (a), (c) – BCS implants fixed in the nasal cortex; (b), (d) – TPG implants fixed in the second nasal cortex with compression in the trabecular area. 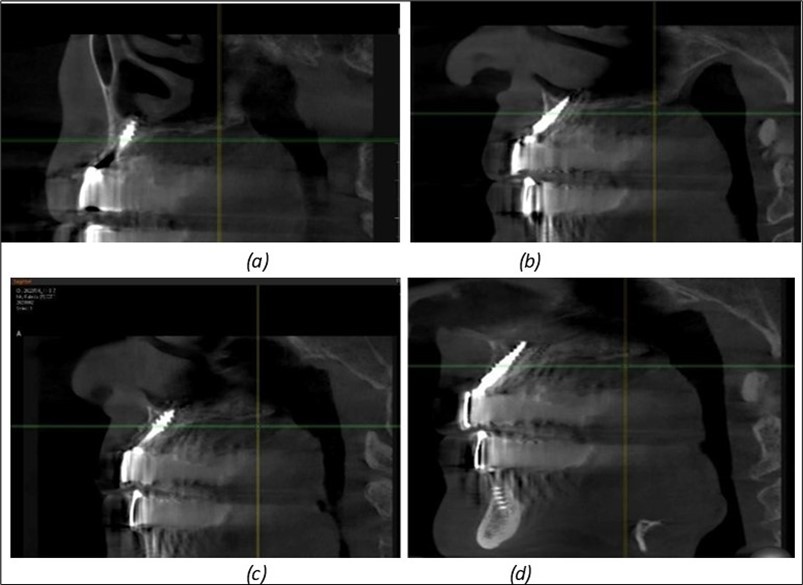
Download figure
Figure 12. Implants fixed distally in quadrant 4 with fixation at the level of the mylohyoid line: (a) The most distal implant fixed in unaffected bone from the previous restoration; (b) The implant fixed in the area where the two stage implant was removed. 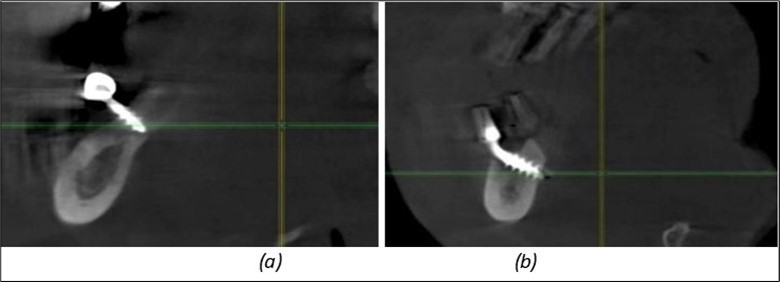
Download figure
Figure 13. Corticobasal BCS implants fixed between the vestibular and lingual cortices with support on the basal bone: (a) BCS fixed between the lateral cortices; (b) BCS implant with support on the basal cortex. 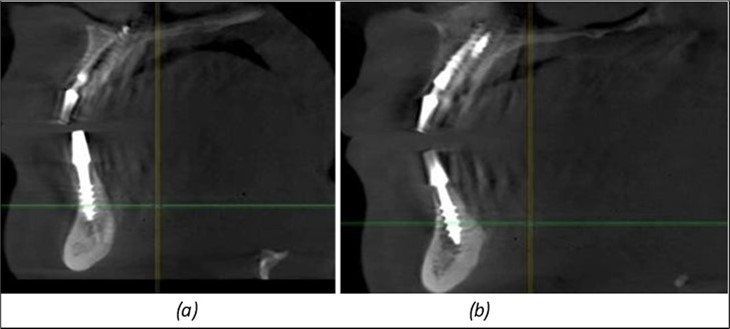
Download figure
Figure 14. Rx panoramic final situation control: (a) Panoramic X-ray with the addition of a distal BCS implant in quadrant 3 at 11.2022; (b) Control X-ray, 10.2023. 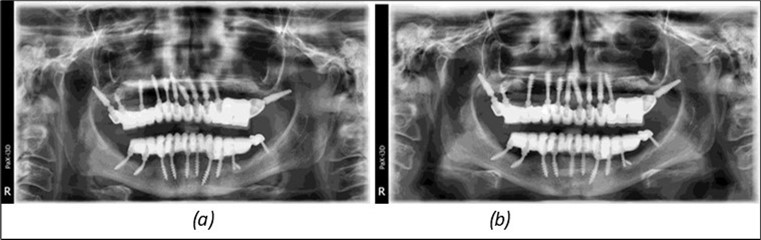
Download figure
Figure 15. Follow-up panoramic X-ray 09.2025 
Download figure
Results
The results of rehabilitation treatment with corticobasal and compressive implants with a polished surface after the failure of two stage implants were highlighted over a period of 3 years and 3 months as being very good (Figure 14, Figure 15), with the patient completing a satisfaction survey in this regard. Certainly, it is necessary to continuemonitoring these results in the long term.
The following aspects were evaluated regarding the results:
-Patient satisfaction related to aesthetics, mastication, and phonation.
-Hygiene capability at the junction between the prosthetic restoration and implants.
Discussion
When the patient is treated with implants on segments and the remaining teeth remainhave questionable stability due to bone resorption, endodontic treatments, andperiodontitis, these implants will absorb all the masticatory forces. This can lead tomechanical overloading and eventual loss of native bone support, with the secondaryappearance of periimplantitis. As long as the teeth are incorporated into the maxillarybones, they are not rigidly connected to the maxillary/mandibular bone. The mechanicalprinciples governing them differ from those of implants, where the implant-boneconnection is rigid.
After the extraction of natural teeth, the bridges on corticobasal implants become anintegral part of the bone, which facilitates the control of the functional situation. Only after all natural teeth are extracted does the bone-implant-prosthesis system(BIPS®) strictly follow the bone's principles. When BIPS® is installed in a mixed systemwhere natural teeth are still present, the situation becomes significantly harder tocontrol.
Natural teeth, bridges supported by teeth, and implant-supported bridges each presentdifferent levels of stability and reliability. Natural teeth, especially when independent,have inherent mobility due to the periodontal ligament – they can experienceelongation, intrusion, or tilting. Bridges supported by teeth may gradually become moremobile, a change often unnoticed by the patient. This leads to the development of amore unilateral chewing pattern.
The differences between natural teeth, tooth-supported bridges, and implant-supportedbridges can compromise the performance of the implant system and may ultimately leadto failure. In the presented case, part of the primary failure was due to the incorrectevaluation of the remaining dental support.
Retreatment with compressive and corticobasal implants is an immediate, accessiblesolution that should also be considered as the first treatment option, provided theremaining teeth is properly assessed. Ideally, the use of a complete solution forthe maxillary and mandibular arches with implants should be utilized, as this willconsiderably reduce the possibilities of later failure.
To control the chewing pattern, it is recommended to place an equal number offunctional teeth on each side of the oral cavity. In this case, the patient had seven teethon the left side and five on the right side of the maxilla, and seven on the right side andsix on the left side of the mandible in two stage implant treatement. The number of functional teeth for the patient mustbe properly evaluated. There are various options for adjusting the number of usableteeth and the chewing surfaces.
Conclusions
The treatment with corticobasal implants should be the first option for patients withmoderate to severe atrophies. The polished surface of the implant protects againstperiimplantitis in most cases and ensures stability at the contact point between theimplant, native bone, and fixed/movable gingiva if the final prosthetic is cemented in short time (3-4) days and content this implants. In the same time lingualized occlusion will keep the forces in the interior of the masticatory poligon. Long term success can be achieved just in case of bone-implant-support (BIPS) it is propert dunn.
Informed consent statement
Considering Romanian Law no. 46/2003 on patients’ rights, Articles 90 and 20, I hereby give my consent to participate as a patient in scientific research and medical education courses, as well as to be photographed and filmed pre-, intra-, and post-operatively, all of these being used for educational, medical, and scientific purposes. -signed by patient
References
- 1.Ihde S, Ihde A, Sipic O. (2022) Pałka Ł.Peri-Implantitis: A new definition proposal based on unnatural spatial arrangement and late mechanical coupling between two cortical bone layers during osseointegration phase. Part I. Applied Sciences. 12(9), 4317-10.
- 2.Álvarez-Camino J C, Valmaseda-Castellón E, Gay-Escoda C. (2013) Immediate implants placed in fresh sockets associated to periapical infectious processes: a systematic review.Med Oral Patol Oral Cir Bucal.18(5):e780–e785. , doi: 10-4317.
- 3.Testori T, Clauser T, Saibene A M, Artzi Z, Avila-Ortiz G et al. (2022) Radiographic protrusion of dental implants in the maxillary sinus and nasal fossae: a multidisciplinary consensus utilising the modified Delphi method.Int. , J Oral Implantol 15(3), 265-275.
- 4.Ragucci G M, Elnayef B, F Suárez-López Del Amo, Wang H L, Hernández-Alfaro F et al. (2019) Influence of exposing dental implants into the sinus cavity on survival and complications rate: a systematic review.Int J Implant Dent.5:. 32-10.
- 5.Antonina I, Lazarov A, Gaur V, Lysenko V, Konstantinovic V et al. (2020) Consensus regarding 16 recognized and clinically proven methods and sub-methods for placing corticobasal® oral implants.Ann Maxillofac Surg.10:. 457-462.
- 6.Lazarov A.Immediate functional loading: results for the concept of the Strategic Implant®.Private Oral Implant Center Aldent. , Sofia, Bulgaria
- 7. (2022) Implant Foundation. 8th Consensus document on indication and procedures for corrective interventions with Cortico-basal® implants. Available from:www.implantfoundation.org.
- 8.Fodor C R, Cretu R, Purghel T.Implant rehabilitation with Strategic Implant® technology in two-stage implants – bone addition, sinus-lift failure.
- 9. (2024) Implant Foundation. 9th Consensus document on indication for tooth extraction and oral implant placement with Cortico-basal® implants. Available from:www.implantfoundation.org.